
Why do people bully?
/

Remedies, Research, Experience, Knowledge, Discussions,

 Research
Research
Robert T Mathie1*, Suzanne M Lloyd2, Lynn A Legg3, Jürgen Clausen4, Sian Moss5, Jonathan RT Davidson6 and Ian Ford2
* Corresponding author: Robert T Mathie rmathie@britishhomeopathic.org
1 British Homeopathic Association, Luton, UK
2 Robertson Centre for Biostatistics, Institute of Health and Wellbeing, University of Glasgow, Glasgow, UK
3 Department of Biomedical Engineering, University of Strathclyde, Glasgow, UK
4 Karl und Veronica Carstens-Stiftung, Essen, Germany
5 Homeopathy Research Institute, London, UK
6 Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, NC, USA
For all author emails, please log on.
Systematic Reviews 2014, 3:142 doi:10.1186/2046-4053-3-142
The electronic version of this article is the complete one and can be found online at: http://www.systematicreviewsjournal.com/content/3/1/142
| Received: | 26 June 2014 |
| Accepted: | 12 November 2014 |
| Published: | 6 December 2014 |
© 2014 Mathie et al.; licensee BioMed Central.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
A rigorous and focused systematic review and meta-analysis of randomised controlled trials (RCTs) of individualised homeopathic treatment has not previously been undertaken. We tested the hypothesis that the outcome of an individualised homeopathic treatment approach using homeopathic medicines is distinguishable from that of placebos.
The review’s methods, including literature search strategy, data extraction, assessment of risk of bias and statistical analysis, were strictly protocol-based. Judgment in seven assessment domains enabled a trial’s risk of bias to be designated as low, unclear or high. A trial was judged to comprise ‘reliable evidence’ if its risk of bias was low or was unclear in one specified domain. ‘Effect size’ was reported as odds ratio (OR), with arithmetic transformation for continuous data carried out as required; OR > 1 signified an effect favouring homeopathy.
Thirty-two eligible RCTs studied 24 different medical conditions in total. Twelve trials were classed ‘uncertain risk of bias’, three of which displayed relatively minor uncertainty and were designated reliable evidence; 20 trials were classed ‘high risk of bias’. Twenty-two trials had extractable data and were subjected to meta-analysis; OR = 1.53 (95% confidence interval (CI) 1.22 to 1.91). For the three trials with reliable evidence, sensitivity analysis revealed OR = 1.98 (95% CI 1.16 to 3.38).
Medicines prescribed in individualised homeopathy may have small, specific treatment effects. Findings are consistent with sub-group data available in a previous ‘global’ systematic review. The low or unclear overall quality of the evidence prompts caution in interpreting the findings. New high-quality RCT research is necessary to enable more decisive interpretation.
Individualised homeopathy; Meta-analysis; Randomised controlled trials; Systematic review
http://www.systematicreviewsjournal.com/content/3/1/142
by Dr. Toni Bark Facebook Page
I trained as a pediatric intern at Bellevue NYU and then in Rehab medicine. I quickly was offered the directorship of the pediatric emergency room at Michael Reese Hospital in Chicago.
While I had initially been furious if parents came in and were not up to date on their children’s vaccines, this attitude changed. And changed drastically.
I began to see patterns. Children who were seen in the vaccine clinic would then come to our ER with seizures, respiratory arrest and asthma attacks. I began to realize, not all children respond well to vaccination and in fact, some die.
It wasn’t until my masters program in disaster management at BU, which I began in 2010 and finished in 2012, did I begin to see the fraudulent nature of how vaccines are being marketed and the corruption in the advisory committees.
I had not even been made aware of the federal vaccine court. I had no idea vaccine recipients who were damaged or killed from vaccines had zero recourse with the manufacturer or physician.
Vaccine manufacturers enjoy full immunity from law suits of any kind, including defective design (as opined by Scalia in Feb 2011) as they are legally listed as “unavoidably unsafe”.
The vaccine court is almost a secret. They have paid out 3 billion dollars since it’s inception in 1986. The vaccine adverse events reporting system is also not well advertised and the government admits it probably only receives 10 percent of the adverse events which occur.
We mandate more vaccines than any other country. We also have the worst infant mortality rate of any first, second, and even some third world countries.
I am 55, so I only received a handful of vaccines. Today, infants receive 14 different vaccines by age of 1 and by age 18, that number is 58 and in some states with flu vaccine mandates, that number is much higher.
A note on the flu vaccine mandates. New Jersey and Connecticut were the first states to mandate flu vaccine for all preschoolers and school age children, annually. This has done nothing to reduce flu cases in their states.In fact, both states are in the highest grouping for flu every year.
While most people do just fine with vaccination, a small percentage do not. And I mean, really do not. Vaccination product inserts describe encephalitis as a possible outcome along with guillan barre paralysis.
Most parents or doctors (for that matter) do not start out “anti-vaccine”, their stance is changed once they have a child who is permanently and profoundly damaged by a vaccine. They then decide no more for that child and no more for their next children.
And they are correct in making that decision.
Genetics, epigenetics and timing can have a great influence on vaccine adverse events. No one drug at one dose is right for everyone and to assume it is, is foolishness.
It is evident from numerous federal cases against many pharmaceutical companies, drug study data is hidden, manipulated and even manufactured. Why is this hard to believe when it comes to vaccine studies?
While I wrote for my masters, I uncovered serious issues with vaccine trials, safety, being one of them. All vaccine safety studies are using false placebos to compare adverse events. The HPV vaccine (which is no longer governmentally recommended in Japan, France and Israel due to serious reactions including deaths) used the new aluminum adjuvant as the placebo. The Prevner safety study, used an experimental meningitis C vaccine.
All the independent Cochrane meta-analysis on vaccine studies end the same way: safety studies are needed in order to assess risk/benefit ratios. There are over 200 new vaccines in the pipeline and as those before them, they will all be approved and recommended which will turn to mandates. When is enough, enough?
After Nazi Germany, the Nuremberg laws were changed to forbid forced medical procedures. The Helsinki accord is very clear; all patients have the right to informed consent prior to medical procedures.
There is no informed consent for vaccination as it is, we really should not be moving backwards.
I am more than willing to send you any studies, to speak to you, or even to fly out and give a presentation.
Watch the Movie Bought for FREE for a limited time.
Dr. Bark received her Bachelor of Science degree in Psychology from The University of Illinois in 1981 and her medical degree from Rush Medical School in 1986.
Dr. Bark completed her Pediatric Residency training at the University of Illinois, Chicago, in 1991, and trained at New York University in Pediatrics from 1986 through 1987 and Rehabilitation Medicine from 1987 through 1988. Immediately post-residency, Dr. Bark worked as attending staff in the Neo-Natal Intensive Care Unit at Michael Reese Hospital. She then took a position as the Director of the Pediatric Emergency Room at Michael Reese Hospital until 1993 when her commitment to natural remedies led her to begin her study of Holistic Medicine.
She has maintained a private practice in Homeopathy for more than fifteen years and was the Medical Director for the integrative Medicine department of Advocate Health Care Systems at Good Shepherd Hospital from June of 2000 until July of 2003.
In 2012 Dr. Bark was bestowed the honor of becoming the 2nd Vice President of the American Institute of Homeopathy (AIH). She also received her Masters in Healthcare Emergency Management (MHEM) from Boston University Medical School that same year.
- See more at: http://vaccineimpact.com/2015/dr-toni-bark-m-d-do-not-remove-vaccine-exemptions-some-children-die-from-vaccines/#sthash.oGJzwTfZ.dpuf
http://vaccineimpact.com/2015/dr-toni-bark-m-d-do-not-remove-vaccine-exemptions-some-children-die-from-vaccines/
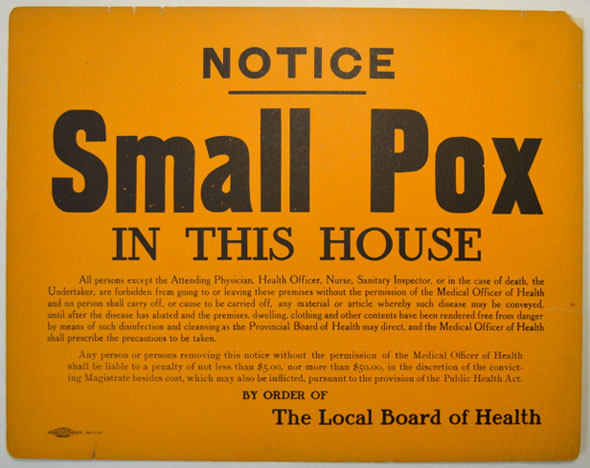
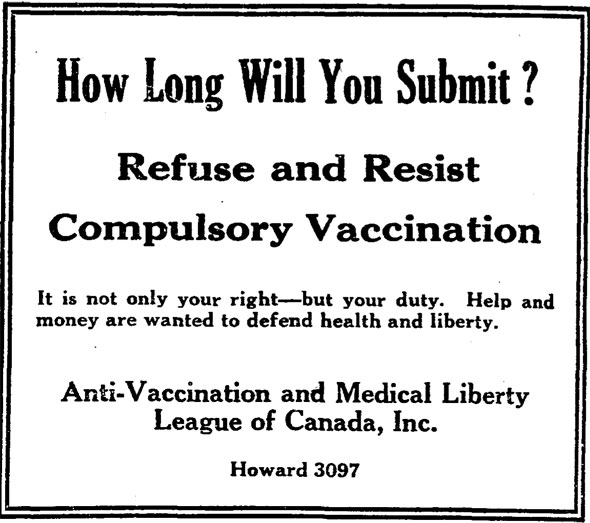
On November 13, 1919, a couple of hundred protesters gathered on the steps of City Hall to air their discontent with the city's compulsory vaccination program. Since 1914, Toronto had been allowed by the province to vaccinate school children against smallpox in the event of an outbreak, with or without the permission of parents. The organizers of the rally, the Toronto branch of the Anti-Vaccination League, had been active for at least 20 years prior to the event. Their notices first appeared in the classified sections of newspapers alongside ads for "pretty, wealthy Canadian girls" looking for husbands and gypsy astrologists.
Some notices advocated for homeopathic vaccinations. "Homeopathic practice is admitted to be very efficient in curing every form of disease, while their medicines are the antithesis of the crude drugs used by [then-Toronto Medical Officer of Health] Dr. Sheard and co.," a reader wrote to the editor of the Toronto Daily Star in October, 1901.
The smallpox vaccine was first developed in the late 16th century by English doctor Edward Jenner. In 1796, the rural physician tested reports that dairy workers had become immune to smallpox after suffering from cowpox, a similar but considerably less lethal disease. By injecting humans with live cowpox, Jenner was able to trigger an immune response that protected the patient against smallpox, one of the great killers of the time.
Jenner also coined the term vaccine from the Latin word "vacca" for cow.
 In the early 1900s, the Anti-Vaccination League stoked fear of immunization by conjuring images of unsanitary animals and horrific side effects. One mother claimed her blind son, who was told by doctors he might recover, had had his hopes dashed following immunization.
In the early 1900s, the Anti-Vaccination League stoked fear of immunization by conjuring images of unsanitary animals and horrific side effects. One mother claimed her blind son, who was told by doctors he might recover, had had his hopes dashed following immunization.
In 1919, shortly after the end of the first world war, the anti-vaccination movement returned to the scene following an epidemic of smallpox that resulted in 2,800 infections. As a result, Dr. Charles Sheard, Toronto's Medical Officer of Health that year, ordered children receive compulsory shots, much to the League's disgust.
 "Vaccination is simply the old scientific absurdity of using disease to fight disease," J. W. Nimmo from the League told a meeting in Earlscourt. Dr. Henry Becker, a prominent homeopathic doctor, claimed vaccines were "made from the grease taken from the heels of horses, from swine pox, and even from dead bodies." This was untrue,Toronto's vaccines were produced at Connaught Laboratories near Steeles and Dufferin from specially kept cows.
"Vaccination is simply the old scientific absurdity of using disease to fight disease," J. W. Nimmo from the League told a meeting in Earlscourt. Dr. Henry Becker, a prominent homeopathic doctor, claimed vaccines were "made from the grease taken from the heels of horses, from swine pox, and even from dead bodies." This was untrue,Toronto's vaccines were produced at Connaught Laboratories near Steeles and Dufferin from specially kept cows.
Among the most prominent opponents to compulsory vaccination were Mayor Thomas Church and Controller Sam McBride. After being told a similar immunization policy in Germany had still resulted in thousands of smallpox deaths, McBride said it was "a pity they weren't all vaccinated. We should have fought them with vaccine points instead of bayonets."
Dr. Sheard said opposition to compulsory vaccination was "absurd" and "puerile."
Nevertheless, the protestors on the steps of City Hall that November urged aldermen to "stop the slaughter of innocents."
The city eventually acquiesced and ended compulsory vaccination, but not before the 1919 outbreak had been largely contained.
Today, parents are still allowed to opt out of vaccinations.
Chris Bateman is a staff writer at blogTO. Follow him on Twitter at @chrisbateman.
Images: City of Toronto Archives
http://www.blogto.com/city/2015/02/a_brief_history_of_anti-vaccination_in_toronto/
Some information that I found interesting. Some things may seem relevant, some random. Take your pick.
Biology (Polio, Lipids, Myelin Sheath, and Meninges)
Poliomyelitis was the term used by doctors to describe the condition in which the gray (polios) anterior matter of the spinal chord (myelos) was inflamed (-itis). 90-95% of reported Polio infections cause no symptoms and leave the host with a life time immunity.
At its peak, Polio was most prevalent in school aged children. Between 5 and 10% of those infected with Poliomyelitis do experience symptoms such as fever, headache, vomiting, diarrhea, stiffness or pain in the arms or legs. 95% of children who experience symptoms are usually back to normal within 3-4 days or up to two weeks when muscle weakness is experienced. However, up to 5% of cases in which children do experience symptoms, result in death. The death rate in adults experiencing symptoms is higher, between 15 and 30%. (1)
Normally, the Poliovirus enters the body, goes to the gut, and begins reproducing. 90-95% of the time this viral infection is short lived because the immune system is designed to send antibodies to fight the virus, just as it would with a common cold.
But, in rare cases, the virus penetrates the central nervous system, causing meningitis. Contrary to the popular understanding, meningitis is not a virus. Meningitis is an event defined by any virus or bacteria penetrating the protective layer of the Central Nervous System and creating inflammation. The CNS is normally protected by 3 durable membranes called the meninges. The Poliovirus only breaches this membrane in approximately 1% of cases. When this happens the patient develops nonparalytic aseptic meningitis, with symptoms of headache, neck, back, abdominal and extremity pain, fever, vomiting, lethargy, and irritability. Similarly, Polio related paralysis occurs only if the virus penetrates the myelin sheath which protects the nerve cells. (32)
The Myelin Sheath and the Meninges are protected and strengthened by phospholipids. Lipids account for 40% of the organic matter in a healthy human body. Phospholipids are abundant in breastmilk, Grass-fed dairy, grass-fed beef, bovine liver, and free range eggs.
“Phospholipids serve as barriers for your cells and have a role in other specialized functions as well. Dipalmitoylphosphatidylcholine is the phospholipid responsible for helping your lungs expand during breathing. Cephalin is a phospholipid in your brain’s white matter, neural tissue, nerves and spinal cord. Sphingomyelin, another phospholipid, is a source of ceramide, one of the substances your body needs to kill defective cells. Lecithin is one of the components of bile, a substance your liver produces to help with digestion.” (53)
Phospholipids play a vital role in the myelinization of the central nervous system. Infants who lack phospholipids (abundantly available in breast milk but not in formula or pasturized cows milk) in their diet have abnormally unstable myelin and a higher propensity to breakdown of the myelin in early adulthood. Adults who lack nutrition high in phospholipids are at increased risk of myelin sheath deterioration.(25)
HISTORY
1870 * “During the rapid urbanization and industrial development, high rates of female employment in poorly paid and casual work, domestic over-crowding, adulterated and contaminated milk all posed enormous threats to the survival of the newborn in the nineteenth century… While physicians, philanthropists, politicians and public health professionals were unanimous in their support of breastfeeding, they were forced to search for substitutes for mothers’ milk, to save those infants whose mothers would not or could not nurse them… The application of chemistry and microscopy to an understanding of the composition of milk laid the foundations for the development of artificial feeds, and food technology, and nutritional science began to inform the theory and practice of infant feeding. By the end of the century simple infant milk formulas were becoming available, and wet nursing was undermined by dry nursing.” (43)
1880 * Canned foods first became available for the public to purchase. (45)
1884 * Evaporated Milk is patented. (49)
1885 * Dr.Pepper was created in Waco, Texas. (49)
1886 * CocaCola was created. (49)
1890 * Increasing numbers of cattle farmers were moving to feed lot style ranches necessitating that cattle be fed increasingly grain-based diets rather than free range grass-based diets. (46) * The outcome was that the resulting beef and dairy products contained far less of the omega-3 and conjugated linoleic acid (CLA) necessary for healthy myelin sheath production. (47)
1893 * The Panic of 1893 was, at the time, the worst economic depression the United States had ever experienced. Many women and children were abandoned by husbands who had lost jobs, wealth, and hope. As a result, many turned to bottle feeding their infants so that they could share child care and look for work. Good nutrition was rare so that even breastfed infants were not likely to get needed fats (lipids) for adequate myelin production. (44)
1894 First US recorded cases of Polio. 132 cases in Vermont. (2)
1906 * It began to gain public attention that foods and medicines had become much more processed and deceptive in the last 50 years. Chemical additives were used to add color, heighten flavor, delay spoilage, soften breads, and more. People who thought they were purchasing strawberry jam found themselves eating strawberry flavored apple scraps, glucose, coal-tar dye, and timothy seed compound that looked and tasted similar to strawberry jam. Questionable producers had begun using adulterated fertilizers, chemicals to cover rancid meat, deodorizer to hide rotten eggs, and substituted less expensive glucose for honey. This concern grew to such a degree that the 1906 Food and Drug Act was passed calling for some degree of government regulation on the labeling of food and medicine.
1909 * Nearly 400 Coca-Cola bottling plants were operating. Some were open only during hot-weather months when demand was high. (68) * The average American consumed 65 pounds of sugar annually. (70)
1910 * Bruce Kraig, professor of history at Roosevelt University and president of the Culinary Historians of Chicago, said “the 1910s saw the beginning of the proliferation of processed foods. In a scant 10 years, Hellmann’s mayonnaise, Oreo cookies, Crisco, Quaker Puffed Wheat and Puffed Rice, Marshmallow Fluff and Nathan’s hot dogs took a bow. Aunt Jemima’s smile was already imprinted upon the American culinary psyche, as were the Kellogg’s and C.W. Post’s brand names.” (70)
1913 * Mississippi was the last state to enact compulsory school attendance laws which had begun in some states as early as 1852. (59)
1914 * The average family spent 60% of their income on food. (45) * Margarine made with vegetable oils and animal fats began to replace butter, greatly reducing the average person’s intake of Vit K2, CLA, Butyrate, and Omega3 (which help prevent cancer, lower body fat, fight inflammation, and strengthen the Myelin sheath). (48)
1916 Reported: 27,000 cases of Polio in the US. (3) * New York City experienced the first large epidemic of polio with over 9,000 reported cases, resulting in 2,343 deaths, out of a population of more than 5 million. This meant that, in New York City, 1 in 550 people contracted Polio and 1 in 2,134 died. (3) * Nationwide there were 27,000 total reported cases and 6,000 deaths out of a US population of 102 million. Or 1 in 3778 contracting polio with 1 in 17,000 resulting in death. (3) * The most serious cases were commonly found in areas with poor nutrition and sanitation such as the densely packed New York City.
1917 * During WWI, women entered the workforce like never before. On the home front, women were employed in factories, stores, and within the government leaving infants and young children in the care of family and friends, thus necessitating a significant rise in the number of bottle fed infants.
1919 * Nutritional foods were in short supply and the government was encouraging Meatless-Mondays, Wheatless Wednesdays, etc.
1920 * Coca-Cola was operating more than 1,000 bottling companies and the drink was found in all but six soda fountains in the US. Some attributed the increased sales to the fact that prohibition had shut down bars. (66, 68)
1922 * Due to contamination of milk supplies, pasteurization became widespread in the United States. Pasteurization destroys Lipase, an enzyme found in milk which is essential to the digestion of fats (lipids). (65)
1923 * Milky Way bar was created. (45)
1929 * The Great Depression cause families to find ways to stretch every bit of food, many spending their days in soup lines when the groceries didn’t go far enough. Even low-lipid grain-fed beef consumption was cut back greatly. (70)
1930 Reported: 9,000 cases. (29) * Snickers bar was created. (45)
1931 Reported: 17,000 cases. (29)
1932 Reported: 3,000 cases. (29) * Mars Bar was created. (45)
1933 Reported: 5,000 cases. (29) * Arthur Kallet and F.J. Schlink authored the national bestseller “100,000,000 Guinea Pigs: Dangers in Everyday Foods, Drugs, and Cosmetics”. They asserted that the American population is being used as guinea pigs in a giant experiment undertaken by the American producers of food stuffs and medicines. Kallet and Schlink premise the book as being “written in the interest of the consumer, who does not yet realize that he is being used as a guinea pig…” (35)
1934 Reported: 7,000 cases. (29)
1935 Reported: 10,000 cases. (29) * KitKat bar was created. (45)
1936 Reported: 4,000 cases. (29) * Spam was invented. (45) * Doctors noted that paralytic poliomyelitis often started at the site of another type of injection. The phenomenon later became known as Provocation Polio. (37)
1937 Reported: 9,000 cases. (29) * Families were spending only 35% of their income on food. (45) * Rolo’s were invented. (45)
1938 Reported: 1,000 cases. (29) * The National Foundation for Infantile Paralysis was created by President Roosevelt and his law partner, Basil O’Connor. (27)
1939 Reported: 7000 cases. (29)
1940 Reported: 10,000 cases. (29)
1941 Reported: 9000 cases. (29) * Drs. Francis and Mack isolated the Mahoney poliovirus “from the pooled feces of three healthy children in Cleveland.” (22)
1942 Reported: 4,000 cases. (29) * Diphtheria and pertussis vaccines were first introduced and cases of paralytic poliomyelitis tripled. (34)
* With the bombing of Pearl Harbor, the US entered into WWII. The government rationed meat, butter, milk, cheese, and eggs (all of the most prominent sources of phospholipids). As a result of these limits, sales of convenience and prepared foods shot up. Margarine became the standard household butter replacement. (70)
1943 Reported: 12,000 cases. (29)
1944 Reported: 19,000 cases. (29) * July 12, Coca-Cola manufactured their one-billionth gallon of Coca-Cola syrup.
1945 Reported: 13,000 cases. (29) * Families were encouraged to plant “Victory Gardens” to fill out the dinner table with vegetables. However, DDT (chlorophenoethane, dichloro-diphenyl-trichloroethane) was a top recommended pesticide recently released in the United States (against the advice of investigators who had studied the pharmacology of the compound and found it dangerous for all forms of life). (71) It would later be classified as a neurotoxin and banned for agricultural use both in the US and worldwide. * Margarine had evolved to a formula completely composed of vegetable oils due to shortages on animal products. (52) * WWII ended. Over 400,000 fathers, sons, and brothers would not be returning from the war. (54) * Spam become a large part of the U.S. soldier’s meat consumption as well as a common household meat on the homefront. Military personnel referred to as “ham that didn’t pass its physical,” or “meatloaf without basic training”. (55)
1946 Reported: 25,000 cases. (29)
1947 Reported: 11,000 cases. (29)
1948 Reported: 26,000 cases. (29) * Jonas Salk, funded by the National Foundation for Infantile Paralysis, set out to determine the number of different types of polio virus. Salk and his team saw this as an opportunity to research the possibility of a vaccine. (19)
1949 Reported: 42,000 cases. (29) * Research showed that Polio struck the hardest in summer months. Dr. Benjamin Sandler, a nutritional expert at the Oteen Hospital, theorized that there could be a connection between the increase of Polio cases and greater amounts of ice cream, soft drinks, and artificial sweeteners consumed during the summer. He used local media to advise North Carolina residents to decrease their consumption of such products. The people listened and the North Carolina State Health Department reported 2,498 cases of polio in 1948, and only 229 cases in 1949 in spite of a national rise of almost 40%! One company reported ice cream sales in NC to be down by 1 million gallons during the first week following Dr. Sandler’s publishing of the anti-polio diet. This inspired the Rockefeller Milk Trust, which sold frozen products to the area, to work with the soft drink business leaders (who also took a significant hit) to convince the people that Dr. Sandler’s findings were contrived and the Polio drop was a coincidence. The next summer ice cream and soda sales, as well as Polio rates were back to normal. (36)
1950 Reported: 32,000 cases. (29)
1951 Reported: 27,000 cases. (29)
1952 Reported: 57,628 cases (The peak year for Polio). *This was 58 years after first reports in the US. (4,5)
1953 Reported: 35,592 cases (3) * A significant drop of 22,000 fewer cases and no vaccine was yet available.
1954, Reported: 38,476 cases. (Up 3,000) (3) * In June of 1954, the first small scale trials with Salk’s vaccine began (2) . The Salk’s Polio strain had been inactivated with formaldehyde (21) and required 4-5 weeks to trigger immunity in the average person. * Six months before Salk’s vaccine test for safety and effectiveness would be reviewed the Polio Fund in the U.S. had already contracted to purchase enough of the Salk vaccine to immunize 9,000,000 children and pregnant women the following year. (15) * Reports claim that Salk’s vaccine was tested for safety and efficiency on 1.8 million children. However, only 443,000 received one or more injections of Salk’s vaccine. 201,229 children received a placebo and 1.2 million children received no vaccination at all and served as a control group. (7, 30) * Despite objections and published concerns by numerous scientist, Harry Weaver, the NFIP’s director of research, wrote: “The practice of medicine is based on calculated risk …. If [we wait until more] research is carried out, large numbers of human beings will develop poliomyelitis who might have been prevented from doing so.” (28) * It turned out that Salk’s “killed-virus” was not as attenuated as he had hoped. Hundreds contracted polio from Salk’s vaccine and many died. (38)
1955, Reported: 28,985 cases. (3) (Down 10,000) * Less than a year later, on April 12th 1955, Salk’s vaccine was declared safe and effective with the field trial results showing that 1 in 1,907 un-vaccinated children contracted Polio while only 1 in 3,964 vaccinated children contracted Polio. In the observed control trials, 1 in 12,333 vaccinated children contracted non-paralytic Polio while 1 in 11,788 unvaccinated children contracted non-paralytic Polio. (30) * Prior to 1955, Polio, Coxsackie virus, and Meningitis (caused by any virus or bacteria) were all diagnosed and reported as Polio based on symptoms. After the field test of Salk’s virus they were redefined as three separate illnesses with specific diagnostic parameters and began to be reported as such. (17) * The first commercial inactive polio vaccines (IPV’s) were being produced by 5 different labs. An American virologist and epidemiologist named Bernice Eddy and her team were assigned to test the vaccines from each company. She discovered that the inactivated vaccine manufactured by Cutter Laboratories contained residual live poliovirus, resulting in the test monkeys showing polio-like symptoms and paralysis. Eddy reported her findings to William Workman, head of the Laboratory of Biologics Control, but her findings were never given to the vaccine licensing advisory committee. (9) The vaccine rolled out anyway. * A few weeks after the press conference announcing success of the vaccine trials, an Idaho doctor reported a case of paralytic polio in a recently vaccinated girl. In the following weeks, more reports came in to local health authorities. All involved a disturbing detail: paralysis began in the vaccinated arm, rather than in the legs as was more common. It was traced back to the Cutter Laboratory batches of the vaccine. (6) * Children who contracted Polio from the Cutter batches were more likely to suffer severe and permanent paralysis, require breathing assistance from and Iron Lung, and more likely to die than children affected with natural polio. (13)
1956 Reported: 15,110 cases. (3) (Down by 14,000 cases)
1957 Reported: 5,185 cases. (3) (Down by 10,000) * At this point more than 100 million doses of Salk’s vaccine had been distributed throughout the United States. (11) * After reports of Polio being contracted from the vaccine and Polio cases contracted by multiple associates of those who had received the vaccine became so numerous that they could no longer be ignored, it came out that the batches issued in 1955 differed from those used in Salk’s trials in that Salk’s original field tested vaccine had included Methiolate and the ones being dispensed to the public did not. (31) * While Salk’s vaccine was inactivated, Dr. Albert Sabin, an American physician and microbiologist, was working to create a live attenuated vaccine because the immunity of Salk’s vaccine was showing evidence of waning and live virus would produce a more natural immunity. However it was also more dangerous to inject people with a live vaccine. To achieve the optimal virulence, he had to isolate the 3 poliovirus strains and then pass them through a myriad of host cells. Sabin’s oral polio vaccine (OPV) is composed of 3 strains. Type 1 evolved from Drs. Francis and Mack’s Mahoney poliovirus from 1941 and had been passaged through no less than 69 monkey cultures, mostly testicular and kidney. (20) * “The resulting material was called Sabin Original Merck (SOM) and was provided to Lederle in 1960 as the seed material to manufacture its polio vaccine. Types II and III were created in a similar fashion.” (22) * He hoped to stimulate a true immune response using a weakened, or attenuated, live virus. He eventually encountered a strain of the polio virus which would infect the intestinal tract but appeared to be to weak to penetrate the myelin sheath of the central nervous system. He had experimented on thousands of monkeys to find the virus but the initial human trials would be carried out in foreign countries. (38, 39)
1958 Reported: 5,787 cases (3) (Up by 600) I * Sabin’s vaccine was given permission for trials in the United States but it was found that people who received Sabin’s oral polio vaccine (OPV) shed weakened virus in their fecal waste for up to 6 weeks, infecting family memebers. (38, 39)
1959 Reported: 8,425 cases. (3) (Up by 2,500) * The US used 79 million pounds of DDT in one year. (72)
1960 Reported: 3,190 cases (3) (Down by 5000) * Ben Sweet and Maurice Hilleman published results showing cancerous growths in the offspring of rodents injected with Salk’s original polio vaccine but no one listened. (h) * “In May of 1960, Dr. Ratner chaired a panel discussion, at the 120th Annual Meeting of the Illinois Medical Society to review the increasing rise in paralytic polio in the United States. The proceedings were reprinted in the August, 1960, Illinois Medical Journal which exposed the Salk vaccine as a frank and ineptly disguised fraud. One of the experts on the panel, statistician Dr. Bernard Greenberg, who went on to testify at Congressional hearings, revealed how data had been manipulated to hide the dangers and ineffectiveness of the vaccine from the pubic. Dr. Greenberg explained that the perceived overall reduction in polio cases was achieved by changing the criteria by which polio was diagnosed.” (16) * “In the 1950’s, the sophisticated virological techniques of today did not exist. And the technology that existed was rarely available to practicing physicians. Therefore, most diagnoses were based upon clinical observation, not sophisticated virological studies. Since polio was epidemic, most physicians were cavalier in making a diagnosis of “non-paralytic poliomyelitis” in children presenting with vague symptoms of muscle aches, malaise, and fever. Since polio was “going around”, such children must have had polio. . . . Interestingly, as the number of polio cases decreased, the number of meningitis cases increased.” (17)
1961 Reported: 1,312 cases (3) (Down by 2000) * Scientist learned that children exposed to the virus during the first year or two of life still carried some antibodies from the womb and nursing causing them to experience a quick and symptom free bout with the Poliovirus conferring lifetime immunity. Modern sanitation practices had eliminated the potential for early exposure meaning that more children were having their first bouts with the virus without the antibodies that were present in the first year of life. (51)
1962 Reported: 886 cases (3) * Virologist Bernice Eddy described the SV40 (vacuolating virus) oncogenic function in inducing sarcoma and tumors in the central nervous system of hamsters inoculated with monkeys cells infected with SV40. (12) Again, it was published and dismissed. * In July, scientist collect lung tissue from an aborted female which were used as a host to produce the WI-38 cell line used in the MMR vaccine development. (61) * Dr. Bernard Greenberg, a biostatistics expert and chairman of the Committee on Evaluation and Standards of the American Public Health Association, testified at a panel discussion used as evidence for the congressional hearings on the Salk’s vaccine. During these hearings he highlighted many problems associated with polio statistics. He pointed out that the recent decline in reported Polio cases were likely the result of changes in the diagnostic requirements for Polio, “Prior to 1954 any physician who reported paralytic poliomyelitis was doing his patient a service by way of subsidizing the cost of hospitalization and was being community-minded in reporting a communicable disease. The criterion of diagnosis at that time in most health departments followed the World Health Organization definition: ‘Spinal paralytic poliomyelitis: signs and symptoms of nonparalytic poliomyelitis with the addition of partial or complete paralysis of one or more muscle groups, detected on two examinations at least 24 hours apart.’ Note that ‘two examinations at least 24 hours apart’ was all that was required. Laboratory confirmation and presence of residual paralysis was not required. In 1955 the criteria were changed to conform more closely to the definition used in the 1954 field trials: residual paralysis was determined 10 to 20 days after onset of illness and again 50 to 70 days after onset…. This change in definition meant that in 1955 we started reporting a new disease, namely, paralytic poliomyelitis with a longer-lasting paralysis. Furthermore, diagnostic procedures have continued to be refined. Coxsackie virus infections and aseptic meningitis have been distinguished from paralytic poliomyelitis. Prior to 1954 large numbers of these cases undoubtedly were mislabeled as paralytic poliomyelitis. Thus, simply by changes in diagnostic criteria, the number of paralytic cases was predetermined to decrease in 1955-1957, whether or not any vaccine was used.” (16) *The same year Salk’s inactivated vaccine began to be replaced by Sabin’s live vaccine (11) reportedly because it was easier to administer and less expensive to manufacture.
1963 * Subsequent studies demonstrated that SV40, which was used in Salk’s vaccine, caused brain tumors in animals (24) and that SV40 could transform or turn cancerous normal human tissue in vitro. * Sabin’s oral “sugar-cube” vaccine became available for general use in spite of the knowledge that the vaccinated individuals would shed a live but weakened Poliovirus for 6 weeks after inoculation. (38, 39)
1964 Reported: 121 cases. (50)
1965 Reported: 61 cases. (50)
1966 * A male fetus was aborted for psychiatric reasons from a 27 year old woman. Fetal lung tissue was removed for the purpose of culturing the origins of the MCR-5 cell line. (14) This cell line would later be used in the DTaP, IPV (Pentacel) as well as 5 other vaccines.
1971 * The USDA moved to ban sodium nitrite because of studies showed connections to pancreatic and bowel cancer, diabetes, and red blood cell damage, but the meat industry insisted that the chemical was safe and publicly accused the USDA of trying to “ban bacon.” (56)
1972 * DDT is banned for agricultural use in the US. (57) * This was be followed by a worldwide ban in the Stockholm Convention in 2001. (58) * The Agency for Toxic Substances & Disease Registry lists developmental processes, endocrine glands and hormones, liver function, the central nervous system, and reproductive systems as areas that are adversely affected by DDT. (72)
1978 * Enhanced Potency IPV produced in human diploid cells was created with the goal of decreasing the number of vaccinations required for lifetime immunity from 4 down to 2 or 3.
1979 * The last recorded case of “wild Polio” in US. All further reports have been vaccine shed strains. (2) * Between 1980 and 1999 there would be 162 confirmed cases of Vaccine induced (or shed) Paralytic Polio in the United States.
1980 * 54% of American women were nursing. (26)
1983 * The CDC recommends 23 doses of 7 vaccines (DPT, MMR, polio) between two months and age six. (63)
1986 * The National Childhood Vaccine Injury Act was passed by Congress to reduce the potential financial liability of vaccine makers due to vaccine injury claims. There had been an recent upturn in adverse reactions to the DTaP vaccine. The company producing the vaccine was losing money so they cut back production. Concerned that reduced production would mean reduced availability of the vaccine, the government created a special Court specifically for dealing with adverse reactions to vaccines. The National Injury Compensation Program was created to provide a no-fault system for compensating vaccine-related injuries or death. Vaccine companies could no longer be held at fault for vaccine related injuries. (60)
1987 * Enhanced potency IPV was released in the US. (18) * The CDC states: “The effect of enhanced-potency IPV on the circulation of poliovirus in a community has not yet been determined, but it is likely to be at least as good as that seen with conventional IPV.” (62)
1992 * A study in Sweden found a 2.5-fold increase in the incidence of meningitis between 1970 and 1980. A case-control study of risk factors for Meningitis conducted in the same area found breastfeeding to be a strong protective factor against Meningitis. (33)
2000 * Due to the fact that Sabin’s OPV could not be given to people with compromised immune systems, it’s ability to cause polio in some recipients, and it’s viral shedding tendency (whereby people exposed to recently vaccinated individuals occasionally contract Polio) the CDC reverted back to recommending that children only be given the Salk’s killed-virus vaccine (IPV) based on previous saftey and efficiency test. Only it wasn’t the same vaccine. The IPV in production was based on Salk’s vaccine but it was in fact the Inhanced Potency IPV released in 87. The CDC recommends 4 doses. (40, 41, 42)
2005 * Inflammation of the Meninges (by any virus including the Poliovirus) is considered Non-Paralytic-Aseptic-Meningitis. (23)
2008 * 70% of women choose to breastfeed. (26) * Studies show evidence that exposure to DDT may be associated with breast cancer, diabetes, decreased semen quality, spontaneous abortion, and impaired neurodevelopment in children. (73)
2014 * The CDC now recommends 49 doses of 14 vaccines before the age of 3 years, more than double what was recommended in 1983. * The CDC recommend 69 doses of 16 vaccines by the age of 18. (63, 64)
Other interesting reads:
National Vaccine Information Center
http://thinkingmomsrevolution.com/dont-vaccinate-protect-cancer-kid/
“A calculated Risk”: the Salk Polio vaccine field trials of 1954 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1114166/
Provocation Polio
http://www.cam.ac.uk/research/features/polio-provocation-the-health-debate-that-refused-to-go-away
Polio, HIV, and Cancer
http://vaxtruth.org/2012/04/the-polio-vaccine-part-3-2/
Vaccines, Abortion & Fetal Tissue
http://www.rtl.org/prolife_issues/LifeNotes/VaccinesAbortion_FetalTissue.html
Human Fetal Cell Lines http://www.ms.academicjournals.org/article/article1409245960_Deisher%20et%20al.pdf
Which Vaccines contain Human Protien and DNA?
http://www.vaccine-tlc.org/human
The benifits of Phospholipid high foods
http://metabolichealing.com/phospholipids-for-tissue-repair-regeneration/
The Polio Vaccine Myth
http://www.vaclib.org/sites/debate/polio.html
Benefits of butter vs. Margarine
http://authoritynutrition.com/butter-vs-margarine/
1. Atkinson W, Hamborsky J, McIntyre L, Wolfe S (eds.) (2009). “Poliomyelitis”. Epidemiology and Prevention of Vaccine-Preventable Diseases (The Pink Book) (PDF) (11th ed.). Washington DC: Public Health Foundation. pp. 231–44.
2. http://amhistory.si.edu/polio/timeline/
3.The Historical Medical Library of The College of Physicians of Philadelphia. Poliomyelitis. U.S. Department of Health, Education, and Welfare. Public Health Service. Health Information Series, No. 8. Public Health Service Publication No. 4. Rev. 1963.
4. Zamula, Evelyn (1991). “A New Challenge for Former Polio Patients”. FDA Consumer 25 (5). Retrieved2010-02-07.
5.“History of Vaccines Website – Polio cases Surge”.College of Physicians of Philadelphia. 3 November 2010. Retrieved 3 November 2010.
6. April 30, 1955 Press Release regarding the investigation into Poliomyelitis Vaccine produced from Cutter Laboratories. Eisenhower Presidential Library.
7. “Competition to develop an oral vaccine”. Conquering Polio. Sanofi PasteurSA. 2007-02-02. Archived from the original on 2007-10-16.
8. Sweet BH, Hilleman MR (November 1960). “The vacuolating virus, S.V. 40″. Proc. Soc. Exp. Biol. Med.105: 420–427. PMID 13774265.
9. Offit, Paul A. The Cutter Incident: How America’s First Polio Vaccine Led to the Growing Vaccine Crisis. Yale University Press, 2007. pp. 62-63.
10. Eddy BE, Borman GS, Berkely WH, Young RD (May 1961). “Tumors induced in hamsters by injection of rhesus monkey cell extracts”. Proc. Soc. Exp. Biol. Med. 107: 191–197.doi:10.3181/00379727-107-26576. PMID 13725644.
11. “World Polio Cut by Salk Vaccine: Safety and Effectiveness of Preventive Confirmed at Geneva Conference”, The New York Times, July 10, 1957
12. Eddy, BE, Borman, GS, Grubbs, GE, Young, RD (May 1962). “Identification of the oncogenic substance in rhesus monkey kidney cell culture as simian virus 40″. Virology17: 65–75. doi:10.1016/0042-6822(62)90082-x.PMID 13889129.
13. Wilson, Daniel J. “The Polio Vaccines of Salk and Sabin”. pg 119
14. J.P. Jacobs et al., “Characteristics of a Human Diploid Cell Designated MRC-5,” Nature 227 (1970): 168.
15. “Polio Fund Buying Salk Vaccine For 9,000,000 Children, Women”, The New York Times, October 19, 1954
16. J.I. Rodale: The Encyclopedia of Common Diseases, Rodale Books Inc., Emmaus Pennsylvania (1962).
17. Congressional Hearings, May 1962; and National Morbidity Reports taken from U.S. Public Health surveillance reports.
18. Atkinson W, Hamborsky J, McIntyre L, Wolfe S, eds. (2008). Epidemiology and Prevention of Vaccine-Preventable Diseases (The Pink Book) (PDF) (10th ed. (2nd printing) ed.). Washington, D.C.: Public Health Foundation. Archived from the original on 2008-09-24. Retrieved 2008-11-29.
19. Rose DR (2004). “Fact Sheet—Polio Vaccine Field Trial of 1954.” March of Dimes Archives. 2004 02 11.
20. A.B. Sabin, A.B. & L. Boulger, History of Sabin Attenuated Poliovirus Oral Live Vaccine Strains. 1 J. Biol. Stand. 115, 115–18 (1973). The Mahoney virus was isolated in 1941 by Drs. Fancis and Mack.
21. Passaging is defined as successive transfer of an infection through experimental animals or tissue culture. Dorland’s Illustrated Medical Dictionary 1240 (27th ed. 1988).
22. Edward Hooper, The River: A Journey to the Source of HIV and AIDS 200 (1999).
23. Chamberlin SL, Narins B (eds.) (2005). The Gale Encyclopedia of Neurological Disorders. Detroit: Thomson Gale. pp. 1859–70. ISBN 0-7876-9150-X.
24. Ruth L. Kirschstein & Paul Gerber, Ependymomas Produced After Intracerebral Inoculation of SV40 into New-Born Hamsters, Nature, July 21, 1962, at 299–300.
25. http://www.ncbi.nlm.nih.gov/pubmed/797220
26. http://www.nytimes.com/2008/12/28/magazine/28froelich-t.html?_r=0
27. Minutes of the Committee on Immunization, Hershey, Pennsylvania, January 23, 1953. Jonas Salk Papers, Mandeville Special Collections, University of California San Diego, Box 254, Folder 2, page 157.
28. Benison S. Tom Rivers: reflections on a life in medicine and science (an oral history memoir). Cambridge, MA: MIT Press; 1967.
29. Paul Meier. “Safety of the Poliomyelitis Vaccine.” Science 125 (1957) 1067-1071.
30. Thomas Francis, Robert Korn, et al. “An Evaluation of the the 1954 Poliomyelitis Vaccine Trials.” American Journal of Public Health 45 (1955)
31. K.A. Brownleb. University of Chicago. Journal of the American Statistical Assosiation. “Statistics of the 1954 Polio Vaccine Trails”. (1955).
32. Chamberlin SL, Narins B (eds.) (2005). The Gale Encyclopedia of Neurological Disorders. Detroit: Thomson Gale. pp. 1859–70. ISBN 0-7876-9150-X.
33. http://www.ncbi.nlm.nih.gov/pubmed/10195681
34. Lindsay KW, et al. Neurology and Neurosurgery Illustrated. Edinburgh/London/New York: Churchill Livingston, 1986:100. Figure 15.2. Polio incidence rates obtained from National Morbidity Reports.
35. Jackson, J. “The Ergot Controversy: Prologue to the 1938 Food, Drug, and Cosmetic Act” J Hist Med Allied Sci1968; XXIII: 248-257
36. data taken from North Carolina State Health Department figures. [26:146;29].
37. Lambert SM. A yaws campaign and an epidemic of poliomyelitis in Western Samoa. J Trop Med Hyg 1936; 39:41–6.
38. Okonek BM, et al. Development of polio vaccines. Access Excellence Classic Collection, February 16, 2001:1. http://www.accessexcellence.org/AE/AEC /CC/polio.html
39. A Science Odyssey: People and Discoveries. Salk produces polio vaccine.www.pbs.org/wgbh/aso/databank/entries/dm52sa.html
40. Shaw D. Unintended casualties in war on polio. Philadelphia Inquirer June 6, 1993:A1.
41. Gorman C. When the vaccine causes the polio. Time October 30, 1995:83
42. Reuters Medical News. CDC publishes Updated Poliomyelitis prevention recommendations for the U.S., May 22, 2000.
43. http://www.historyandpolicy.org/policy-papers/papers/feeding-babies-in-the-21st-century-breast-is-still-best-but-for-new-reasons
44. Timberlake, Jr., Richard H. (1997). “Panic of 1893″. In Glasner, David; Cooley, Thomas F., eds. Business Cycles and Depressions: an Encyclopedia. New York: Garland Publishing. pp. 516–18.
45. http://www.localhistories.org/food.html
46. http://www.tshaonline.org/handbook/online/articles/aucrw
47. https://www.bulletproofexec.com/grass-fed-meat-part-1/
48. http://authoritynutrition.com/butter-vs-margarine/
49. http://www.localhistories.org/drinktime.html
50. http://www.cdc.gov/vaccines/vpd-vac/polio/dis-faqs.htm
51. Jane Smith, Patenting the Sun: Polio and the Salk Vaccine (New York: William Morrow and Co., Inc, 1990), p. 34.
52. Clark, Paul (6 May 1983). “The marketing of margarine”. Paper presented to a seminar on Marketing and Advertising in the 20th Century at Central London Polytechnic. Emeral Backfiles. p. 54. Retrieved 2009-11-10.
53. http://www.livestrong.com/article/446527-what-are-phospholipids-in-the-diet/
54. Michael Clodfelter. Warfare and Armed Conflicts – A Statistical Reference to Casualty and Other Figures, 1500–2000. 2nd ed. 2002 ISBN 0-7864-1204-6 pp. 584–591
55. Martin, Andrew (November 15, 2008). “Spam Turns Serious and Hormel Turns Out More”. The New York Times. Retrieved May 23, 2010.
56. http://news.google.com/newspapers?nid=1298&dat=19771018&id=Y99NAAAAIBAJ&sjid=BIsDAAAAIBAJ&pg=1754,2504359
57. Linda Lear (1 April 2009). Rachel Carson: Witness for Nature. Mariner Books. ISBN 978-0-547-23823-4.
58. Larson, Kim (December 1, 2007). “Bad Blood”. On Earth (Winter 2008). Retrieved June 5, 2008
59. Katz, Michael S. “A History of Compulsory Education Laws”. ERIC – Institute of Education Sciences. ERIC. Retrieved 19 December 2014.
60. National Childhood Vaccine Injury Act of 1986 (42 U.S.C. §§ 300aa-1 to 300aa-34)
61. http://www.nature.com/news/medical-research-cell-division-1.13273
62. http://www.cdc.gov/mmwr/preview/mmwrhtml/00025216.htm
63. http://www.nvic.org/CMSTemplates/NVIC/pdf/49-Doses-PosterB.pdf
64. http://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-pocket-pr.pdf
65. http://www.ncbi.nlm.nih.gov/pubmed/9602205
66. http://iml.jou.ufl.edu/projects/spring08/Cantwell/20thcent/20-40.html
67. “Coke Can History”. Archived from the original on January 18, 2010.
68. http://www.coca-colacompany.com/our-company/history-of-bottling
70. http://leitesculinaria.com/10348/writings-dining-through-the-decades-american-food-history.html
71. http://jee.oxfordjournals.org/content/38/2/197 (“DDT to Control Corn Flea Beetle” April 1, 1945)
72 http://www.atsdr.cdc.gov/substances/toxsubstance.asp?toxid=20
73. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2737010/
The choice of homeopathic medicine is based on the patient’s specific symptoms and not the disease itself. Because of this, in the first consultation the homeopath will seek a complete and accurate picture of the health status and symptoms of the patient.
The homeopath will ask you about your condition, physical, physiological, mental and emotional. He or she will ask you to describe what factors improve and what factors worsen the symptoms, how you react to heat and cold, different weather, different body positions, etc. He or she will ask you about your food preferences and aversions, how you sleep, your lifestyle and habits, your personality, your medical history and your family’s medical history, etc. The first homeopathic consultation can easily last two hours. Subsequent ones last a shorter time, often half an hour, and usually happen about once a month.
Genotype was determined for 26 of the 29 PCR confirmed cases. All were D8 and 25 of 26 were at least 99.8% identical to the MVs/Taunton.GBR/27.12 sequence-variant. This is the same strain imported toCanada from the Netherlands multiple times during 2013while a large outbreak occurred in that country,leading also to the importation that sparked an outbreak in southern Alberta in the fall of 2013and a family cluster in Fraser East that did not result in further transmission. For one D8 case the similarity to the Netherlands strain is not known.
Remember being a really pissed off angsty teenager? I do! That is how I feel these days! When realizing (yet again) that like my parents told me back then when I yelled 'It isn't fair' and they retorted 'Life isn't fair', I am yet again being proven how true this is...
~Heavy sigh... 
What is it? I'm talking about the mother of all antioxidants, the master detoxifier and maestro of the immune system: GLUTATHIONE (pronounced "gloota-thigh-own").
The good news is that your body produces its own glutathione. The bad news is that poor diet, pollution, toxins, medications, stress, trauma, aging, infections and radiation all deplete your glutathione.
This leaves you susceptible to unrestrained cell disintegration from oxidative stress, free radicals, infections and cancer. And your liver gets overloaded and damaged, making it unable to do its job of detoxification.
In treating chronically ill patients with Functional Medicine for more than 10 years, I have discovered that glutathione deficiency is found in nearly all very ill patients. These include people with chronic fatigue syndrome, heart disease, cancer, chronic infections, autoimmune disease, diabetes, autism, Alzheimer's disease, Parkinson's disease, arthritis, asthma, kidney problems, liver disease and more.
At first I thought that this was just a coincidental finding, but over the years I have come to realize that our ability to produce and maintain a high level of glutathione is critical to recovery from nearly all chronic illness -- and to preventing disease and maintaining optimal health and performance. The authors of those 76,000 medical articles on glutathione I mentioned earlier have found the same thing!
So in today's blog I want to explain what glutathione is, why it's important and give you 9 tips that will help you optimize your glutathione levels, improve your detoxification system and protect help yourself from chronic illness.
What is Glutathione?
Glutathione is a very simple molecule that is produced naturally all the time in your body. It is a combination of three simple building blocks of protein or amino acids -- cysteine, glycine and glutamine.
The secret of its power is the sulfur (SH) chemical groups it contains. Sulfur is a sticky, smelly molecule. It acts like fly paper and all the bad things in the body stick onto it, including free radicals and toxins like mercury and other heavy metals.
Normally glutathione is recycled in the body -- except when the toxic load becomes too great. And that explains why we are in such trouble ...
In my practice, I test the genes involved in glutathione metabolism. These are the genes involved in producing enzymes that allow the body to create and recycle glutathione in the body. These genes have many names, such as GSTM1, GSTP1 and more.
These genes impaired in some people for a variety of important reasons. We humans evolved in a time before the 80,000 toxic industrial chemicals found in our environment today were introduced into our world, before electromagnetic radiation was everywhere and before we polluted our skies, lakes, rivers, oceans and teeth with mercury and lead.
That is why most people survived with the basic version of the genetic detoxification software encoded in our DNA, which is mediocre at ridding the body of toxins. At the time humans evolved we just didn't need more. Who knew we would be poisoning ourselves and eating a processed, nutrient-depleted diet thousands of years later?
Because most of us didn't require additional detoxification software, almost of half of the population now has a limited capacity to get rid of toxins. These people are missing GSTM1 function -- one of the most important genes needed in the process of creating and recycling glutathione in the body.
Nearly all my very sick patients are missing this function. The one-third of our population that suffers from chronic disease is missing this essential gene. That includes me. Twenty years ago I became mercury poisoned and suffered from chronic fatigue syndrome due to this very problem. My GSTM1 function was inadequate and I didn't produce enough glutathione as a result. Eventually, my body broke down and I became extremely ill ...
This is the same problem I see in so many of my patients. They are missing this critical gene and they descend into disease as a result. Let me explain how this happens ...
The Importance of Glutathione in Protecting Against Chronic Illness
Glutathione is critical for one simple reason: It recycles antioxidants. You see, dealing with free radicals is like handing off a hot potato. They get passed around from vitamin C to vitamin E to lipoic acid and then finally to glutathione which cools off the free radicals and recycles other antioxidants. After this happens, the body can "reduce" or regenerate another protective glutathione molecule and we are back in business.
However, problems occur when we are overwhelmed with too much oxidative stress or too many toxins. Then the glutathione becomes depleted and we can no longer protect ourselves against free radicals, infections, or cancer and we can't get rid of toxins. This leads to further sickness and soon we are in the downward spiral of chronic illness.
But that's not all. Glutathione is also critical in helping your immune system do its job of fighting infections and preventing cancer. That's why studies show that it can help in the treatment of AIDS.(i)
Glutathione is also the most critical and integral part of your detoxification system. All the toxins stick onto glutathione, which then carries them into the bile and the stool -- and out of your body.
And lastly, it also helps us reach peak mental and physical function. Research has shown that raised glutathione levels decrease muscle damage, reduce recovery time, increase strength and endurance and shift metabolism from fat production to muscle development.
If you are sick or old or are just not in peak shape, you likely have glutathione deficiency. In fact, the top British medical journal, the Lancet, found the highest glutathione levels in healthy young people, lower levels in healthy elderly, lower still in sick elderly and the lowest of all in the hospitalized elderly. (ii)
Keeping yourself healthy, boosting your performance, preventing disease and aging well depends on keeping your glutathione levels high. I'll say it again ... Glutathione is so important because it is responsible for keeping so many of the keys to UltraWellness optimized.
It is critical for immune function and controlling inflammation. It is the master detoxifier and the body's main antioxidant, protecting our cells and making our energy metabolism run well.
And the good news is that you can do many things to increase this natural and critical molecule in your body. You can eat glutathione-boosting foods. You can exercise. And you can take glutathione-boosting supplements. Let's review more specifics about each.
9 Tips to Optimize your Glutathione Levels
These 9 tips will help you improve your glutathione levels, improve your health, optimize your performance and live a long, healthy life.
Eat Foods that Support Glutathione Production
1. Consume sulfur-rich foods. The main ones in the diet are garlic, onions and the cruciferous vegetables (broccoli, kale, collards, cabbage, cauliflower, watercress, etc.).
2. Try bioactive whey protein. This is great source of cysteine and the amino acid building blocks for glutathione synthesis. As you know, I am not a big fan of dairy. But this is an exception -- with a few warnings. The whey protein MUST be bioactive and made from non-denatured proteins ("denaturing" refers to the breakdown of the normal protein structure). Choose non-pasteurized and non-industrially produced milk that contains no pesticides, hormones, or antibiotics. Immunocal is a prescription bioactive non-denatured whey protein that is even listed in the Physician's Desk Reference.
Exercise for Your Way to More Glutathione
3. Exercise boosts your glutathione levels and thereby helps boost your immune system, improve detoxification and enhance your body's own antioxidant defenses. Start slow and build up to 30 minutes a day of vigorous aerobic exercise like walking or jogging, or play various sports. Strength training for 20 minutes 3 times a week is also helpful.
Take Glutathione Supporting Supplements
One would think it would be easy just to take glutathione as a pill, but the body digests protein -- so you wouldn't get the benefits if you did it this way. However, the production and recycling of glutathione in the body requires many different nutrients and you CAN take these. Here are the main supplements that need to be taken consistently to boost glutathione. Besides taking a multivitamin and fish oil, supporting my glutathione levels with these supplements is the most important thing I do every day for my personal health.
4. N-acetyl-cysteine. This has been used for years to help treat asthma and lung disease and to treat people with life-threatening liver failure from Tylenol overdose. In fact, I first learned about it in medical school while working in the emergency room. It is even given to prevent kidney damage from dyes used during x-ray studies.
5. Alpha lipoic acid. This is a close second to glutathione in importance in our cells and is involved in energy production, blood sugar control, brain health and detoxification. The body usually makes it, but given all the stresses we are under, we often become depleted.
6. Methylation nutrients (folate and vitamins B6 and B12). These are perhaps the most critical to keep the body producing glutathione. Methylation and the production and recycling of glutathione are the two most important biochemical functions in your body. Take folate (especially in the active form of 5 methyltetrahydrofolate), B6 (in active form of P5P) and B12 (in the active form of methylcobalamin).
7. Selenium. This important mineral helps the body recycle and produce more glutathione.
8. A family of antioxidants including vitamins C and E (in the form of mixed tocopherols), work together to recycle glutathione.
9. Milk thistle (silymarin) has long been used in liver disease and helps boost glutathione levels.
So use these nine tips and see how they work to help you optimzie your glutathione levels. When you do, you will take one more step to lifelong vibrant health.
Now I'd like to hear from you...
Had you ever heard of this important nutrient before?
Have you tried any of the advice in this article?
What effects have you noticed on your health?
Please leave your thoughts by adding a comment below.
To your good health,
Mark Hyman, M.D.
References
(i) De Rosa SC, Zaretsky MD, Dubs JG, Roederer M, Anderson M, Green A, Mitra D, Watanabe N, Nakamura H, Tjioe I, Deresinski SC, Moore WA, Ela SW, Parks D, Herzenberg LA, Herzenberg LA. N-acetylcysteine replenishes glutathione in HIV infection. Eur J Clin Invest. 2000 Oct;30(10):915-29
(ii) Nuttall S, Martin U, Sinclair A, Kendall M. 1998. Glutathione: in sickness and in health. The Lancet 351(9103):645-646
Mark Hyman, M.D. practicing physician and founder of The UltraWellness Center is a pioneer in functional medicine. Dr. Hyman is now sharing the 7 ways to tap into your body's natural ability to heal itself. You can follow him on Twitter, connect with him on LinkedIn, watch his videos on Youtube and become a fan on Facebook.
Follow Mark Hyman, MD on Twitter: www.twitter.com/markhymanmd
http://www.huffingtonpost.com/dr-mark-hyman/glutathione-the-mother-of_b_530494.html
Excretion of vaccine strain measles virus in urine and pharyngeal secretions of a child with vaccine associated febrile rash illness;
We describe excretion of measles vaccine strain Schwarz in a child who developed a febrile rash illness eight days after primary immunisation against measles, mumps and rubella. Throat swabs and urine specimens were collected on the fifth and sixth day of illness, respectively. Genotyping demonstrated measles vaccine strain Schwarz (genotype A). If measles and rubella were not under enhanced surveillance in Croatia, the case would have been either misreported as rubella or not recognised at all.
Introduction
Vaccination against measles was introduced into the Croatian vaccination schedule in 1968 for all children at the age of 12 months and at first grade of elementary school. The vaccine containing the Edmonston-Zagreb measles virus strain was produced by the Institute of Immunology, Zagreb. In 1976, the monovalent measles vaccine was replaced by a trivalent measles, mumps, rubella (MMR) vaccine, containing the same Edmonston-Zagreb strain of the same producer. In 2008, 18 cases of vaccine-associated mumps were reported that has resulted from transmission of the mumps component (L-Zagreb) to close contacts of children who had received primary vaccination with this trivalent vaccine [3,4,11]. This vaccine was thereafter replaced by Priorix (GSK; containing the RIT 4385 mumps virus strain and the Schwarz measles virus strain) for the first MMR vaccination in January 2009. The MMR vaccine produced by the Croatian Institute of Immunology is still used for the second dose of MMR. Since the MMR vaccine used for primary vaccination was changed in January 2009, vaccine-associated mumps in contacts of vaccinees have no longer been reported [5].
No suspected measles or rubella cases were reported in Croatia during 2010. In the last five-year period, one local outbreak of rubella occurred in Croatia in 2007, affecting 39 adolescents and one outbreak of measles in 2008, affecting 51 people. The illness in the index cases of both outbreaks was imported. Independently of these two outbreaks, only five cases of measles and another five cases of rubella were reported in Croatia from 2005 to 2009, which were eventually discarded by serology or classified as imported. After receiving information on a measles outbreak in Roma children in Bulgaria in 2009 [6,7] and media reports on rubella cases in neighbouring Bosnia and Herzegovina, the Croatian Institute of Public Health sent a circular letter to healthcare workers in Croatia on 15 March 2010 to raise awareness of possible importations of measles and rubella.
Four suspected rubella cases were notified in Croatia in the second half of March 2010. Three cases were discarded based on negative serology for measles and rubella and lack of epidemiological link to a possible source. One case may have had a chance to be exposed to rubella but also had a history of MMR vaccination and is described here.
Case description
A healthy child (14 months-old) was vaccinated on 9 March 2010 with Priorix MMR vaccine according to the Croatian childhood vaccination schedule. The child had facial erythema without fever on 14 March and developed a macular rash and fever on 17 March. It was examined on 21 March at the county hospital and reported as a possible case of rubella to the epidemiology department at the County Institute of Public Health on 23 March.
Since rubella and measles are under enhanced surveillance according to the national action plan for measles and rubella elimination, an epidemiological investigation was initiated, and serum, urine and throat swab specimens for laboratory testing were obtained. The investigation found no similar cases among contacts of the patient. A source of rubella infection was not identified, however, possible exposure to rubella or measles virus could not be completely excluded, because the child had travelled abroad during the two weeks preceding the illness.
A serum sample and throat swabs were taken on 23 March and a urine specimen on 24 March. On 26 March, the rash was still present. Serum was obtained again from the convalescent child on 11 April. In addition, a serum sample from the asymptomatic pregnant mother was obtained on 24 March.
Laboratory investigation
Serologic tests of the patient and mother were performed at the World Health Organization (WHO) national measles laboratory, Virology Department, Croatian Institute of Public Health. For the detection of specific measles and rubella IgM and IgG antibodies we used commercial ELISA (Rubella IgM/IgG: Dia Sorin; Measles IgM/IgG: Genzyme Virotech GmbH). For detection of specific mumps IgM and IgG antibodies, a commercial immunofluorescence test was used (Euroimmun). Throat swab and urine were initially tested for measles virus at the Department of Molecular Diagnostics, Croatian Institute of Public Health using real-time RT-PCR (Applied Biosystems), using the primer/probe set for the measles virus nucleoprotein (N) gene [2].
The child's paired sera were tested in parallel. The first serum tested negative for IgM and IgG antibodies against rubella virus and mumps virus, while measles antibodies were equivocal for IgM and negative for IgG. The child's second serum obtained on 11 April also tested negative for both IgM and IgG rubella antibodies, while measles antibodies were negative for IgM, but IgG-positive, and mumps antibodies were postitive for IgM as well as for IgG. The mother was negative for IgM and positive for IgG antibodies against both measles and rubella virus (the mother’s vaccination status could not be determined with certainty). The child's throat swab was negative in RT-PCR for measles RNA, while the urine tested positive.
An additional RT-PCR was performed, targeting the 3’-end of the N gene [1]. PCR products were obtained from throat swab and urine, sequenced and compared using the BLAST algorithm, and finally identified as Schwarz vaccine strain (genotype A).
Discussion
We demonstrated excretion of the Schwarz measles vaccine virus in a child with a vaccine-associated febrile rash illness in urine and in pharyngeal excretions.
Virus excretion in vaccinees has been reported before [8-10], but to our knowledge, this is documented for the first time for the Schwarz vaccine strain. Interestingly, although the blood for serology testing was obtained 14 and 32 days after vaccination, the child still had no antibodies to rubella virus in either serum sample. It is unclear why there was no seroconversion to rubella 32 days after vaccination, although this is not an unusual finding. The dynamics of measles and mumps antibodies were as expected for someone who had either been vaccinated or had natural infection, indicating that the child did not have impaired antibody production kinetics in general.
According to WHO guidelines for measles and rubella elimination, routine discrimination between aetiologies of febrile rash disease is done by antibody assays, not necessarily by virus detection [12]. However, in a patient recently MMR-vaccinated, only molecular techniques can differentiate between wildtype measles or rubella infection or vaccine-associated disease.
This case report demonstrates that excretion of Schwarz measles virus occurs in vaccinees. Also, it demonstrates a need to strengthen surveillance of measles and rubella cases continuously, also in countries that are currently approaching elimination of measles and rubella.
Competing interests: Maja Santak is an employee of the Institute of Immunology, Zagreb, the national vaccine producer.
References
http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19652
Blaming Homeopaths for people choosing to not vaccinate is like blaming people who sell rubber boots for rain.
Guess what it is called?! 'Too good to be true'
and that might be the essence of it. ...
but wait...
The 'Biology of Belief' (by Bruce Lipton) https://www.youtube.com/watch?v=0MUsg23WDBY says it is so true and 'scientifically so'...
if 'Science Says'...
then...
???
... to be continued (yes like a bad soap opera) ha ;)
Homeopathy has a long history of popular use (hundreds of years). It also has a history of being criticized in North America where the medical industry is dominated by the pharmaceutical industry. Homeopathy is second only to Jesus as the two most controversial topics according to Wikipedia.1
Considering my previous career in political advocacy focusing on environmental and conservation issues, I sometimes ask myself; Is that what attracted me to homeopathy? No! It was the fact that once I gave it a try for my lifetime struggle with de-habilitating eczema, it did something that nothing else could do for me and so I was ecstatic.2 That success indeed was what made me passionate about ensuring that people know about homeopathy as an option if they so choose.
Unfortunately, that passion has led me here – writing to justify the amazing healing that I am now able to do for many others, now that I’ve spent over ten years continuing to study all aspects of homeopathy above and beyond my four year diploma requirement in order to call myself a homeopathic practitioner.3 Luckily I now have access to University level databases of research publications without having to pay the download fees. You, reading this are lucky too, because I am writing to share this with you.
I have been reticent to spend the time to put this type of information out there before now because I realize that there is no way that this article written by a homeopath will ever change the minds of anyone who is bothering to put all their wasted energy in trying to discredit homeopathy. If you are one of those people on a mission to defame individual homeopathic practitioners who are just trying to use their education driven refined skills to help do some good in this world, I have only two requests for you as follows:
SIMPLE right?
Right!
For any others who are going to read further into this bibliography of research on homeopathy, I suggest that if you are not professionally educated in research, research methods, homeopathy or any other health field that you have someone who is to look through these papers for you. I think my reasons should be obvious to you however I will say it outright – if you are not trained and/or highly experienced in homeopathy – you cannot speak as if you are the expert to those who actually are the experts.
In the meanwhile, here are some current research on homeopathic remedies in general.
This literature review was conducted using the EBSCO database including the Academic Search Complete thanks to the University of Central Lancashire. The databases specifically chosen were Academic Search Complete, Medline, Medline with full text, AMED (Allied and Complementary Medical Database, CINAHL Complete, PsycARTICLES, PsycINFO, Social Sciences ABSTRACTS (H.W. Wilson), and SocINDEX with full text. The search method used was the Advanced Search with subject words Homeopathy and Homeopathic Remedies. Unfortunately this search presented 984 items in the search results so the following edits were made. Any publications older than five years were not included. This resulted in 313 publications. While searching through each and every title of this search, I did not include in this bibliography any of the editorials, opinion pieces or individual case studies that showed up in this search which eliminated 18 of them within the first 100 that I looked through so far.
Adler, U. C., Krüger, S., Teut, M., Lüdtke, R., Bartsch, I., Schützler, L., & ... Witt, C. M. (2011). Homeopathy for Depression - DEP-HOM: study protocol for a randomized, partially double-blind, placebo controlled, four armed study. Trials, 12(1), 43-49. doi:10.1186/1745-6215-12-43
Adler, U. C., Krüger, S., Teut, M., Lüdtke, R., Schützler, L., Martins, F., & ... Witt, C. M. (2013). Homeopathy for Depression: A Randomized, Partially Double-Blind, Placebo-Controlled, Four-Armed Study (DEP-HOM). Plos ONE, 8(9), 1-9. doi:10.1371/journal.pone.0074537
Ainsworth, S. (2012). Time to consign homeopathy to the history books?. Practice Nurse, 42(10), 34-35.
Akaeva, T. V., & Mkhitaryan, K. N. (2014). Foundation of concept of constitutional homeopathic remedy by using electropuncture methods. International Journal Of High Dilution Resarch, 13(47), 132-133.
Almirantis, Y. (2013). Homeopathy – between tradition and modern science: remedies as carriers of significance. Homeopathy, 102(2), 114-122. doi:10.1016/j.homp.2013.01.003
Amalcaburio, R., Filho, L. M., Honorato, L. A., & Menezes, N. A. (2009). Homeopathic remedies in a semi-intensive alternative system of broiler production. International Journal Of High Dilution Resarch, 8(26), 33-39.
Arlt, S., Padberg, W., Drillich, M., & Heuwieser, W. (2009). Efficacy of homeopathic remedies as prophylaxis of bovine endometritis. Journal Of Dairy Science, 92(10), 4945-4953. doi:10.3168/jds.2009-2142
Arora, S., Aggarwal, A., Singla, P., Jyoti, S., & Tandon, S. (2013). Anti-proliferative effects of homeopathic medicines on human kidney, colon and breast cancer cells. Homeopathy: The Journal Of The Faculty Of Homeopathy, 102(4), 274-282. doi:10.1016/j.homp.2013.06.001
Banerjee, A., Chakrabarty, S. B., Karmakar, S. R., Chakrabarty, A., Biswas, S. J., Haque, S., & ... Khuda-Bukhsh, A. R. (2010). Can Homeopathy Bring Additional Benefits to Thalassemic Patients on Hydroxyurea Therapy? Encouraging Results of a Preliminary Study. Evidence-Based Complementary & Alternative Medicine (Ecam), 7(1), 129-136. doi:10.1093/ecam/nem161
Banerjee, A., Chakrabarty, S., Karmakar, S., Chakrabarty, A., Biswas, S., Haque, S., & ... Khuda-Bukhsh, A. (2009). Can homeopathy bring additional benefits to thalassemic patients on hydroxyurea therapy? Encouraging results of a preliminary study. Homoeopathic Heritage, 34(4), 33-40.
Beeraka, P. (2009). The pharmacological action of homeopathic remedies. Simillimum, 22(3), 66.
Bell, I. R. (2012). Homeopathy as Systemic Adaptational Nanomedicine: The Nanoparticle-Cross-Adaptation-Sensitization Model. American Journal Of Homeopathic Medicine, 105(3), 116-130.
Bell, I., Brooks, A., Howerter, A., Jackson, N., & Schwartz, G. (2013). Acute Electroencephalographic Effects From Repeated Olfactory Administration of Homeopathic Remedies in Individuals With Self-reported Chemical Sensitivity. Alternative Therapies In Health & Medicine, 19(1), 46-57.
Bell, I. R., Howerter, A., Jackson, N., Aickin, M., Bootzin, R. R., & Brooks, A. J. (2012). Nonlinear dynamical systems effects of homeopathic remedies on multiscale entropy and correlation dimension of slow wave sleep EEG in young adults with histories of coffee-induced insomnia. Homeopathy, 101(3), 182-192. doi:10.1016/j.homp.2012.05.007
Bell, I. R., Howerter, A., Jackson, N., Brooks, A. J., & Schwartz, G. E. (2012). Multiweek Resting EEG Cordance Change Patterns from Repeated Olfactory Activation with Two Constitutionally Salient Homeopathic Remedies in Healthy Young Adults. Journal Of Alternative & Complementary Medicine, 18(5), 445-453. doi:10.1089/acm.2011.0931
Bell, I., Koithan, M., & Brooks, A. (2013). Testing the nanoparticle-allostatic cross-adaptation-sensitization model for homeopathic remedy effects. Homeopathy, 102(1), 66.
Bell, I. R., & Schwartz, G. E. (2013). Adaptive network nanomedicine: an integrated model for homeopathic medicine. Frontiers In Bioscience (Scholar Edition), 5685-708.
Bellavite, P., Magnani, P., Marzotto, M., & Conforti, A. (2009). Assays of homeopathic remedies in rodent behavioural and psychopathological models. Homeopathy: The Journal Of The Faculty Of Homeopathy, 98(4), 208-227. doi:10.1016/j.homp.2009.09.005
Bellavite, P., Marzotto, M., Olioso, D., Moratti, E., & Conforti, A. (2014). High-dilution effects revisited. 2. Pharmacodynamic mechanisms. Homeopathy: The Journal Of The Faculty Of Homeopathy, 103(1), 22-43. doi:10.1016/j.homp.2013.08.002
Carter, J., & Aston, G. (2012). Use of homeopathic Arnica among childbearing women: A survey. British Journal Of Midwifery, 20(4), 254-261.
Chatfield, K., Mathie, R., & Fisher, P. (2011). Comment 2 on: Homeopathy has clinical benefits in rheumatoid arthritis patients that are attributable to the consultation process but not the homeopathic remedy: A randomized controlled trial. Rheumatology (Oxford), 50(8), 1529.
Clayton, L. (2012). Top ten: homeopathic remedies for pregnancy and birth. Essentially MIDIRS, 3(5), 27-31.
Copeland, A. (2011). A STUDY TO DETERMINE THE EFFECTIVENESS OF HOMEOPATHIC WEIGHT LOSS REMEDIES: HCG NON-HCG ~vs~ NON-HCG. Original Internist, 18(3), 107-116.
Csupor, D., Boros, K., & Hohmann, J. (2013). Low Potency Homeopathic Remedies and Allopathic Herbal Medicines: Is There an Overlap?. Plos ONE, 8(9), 1-5. doi:10.1371/journal.pone.0074181
Drozdov, V. V. (2014). Optimization of coprological studies in animals with the use of homeopathic Nux vomica 6CH. International Journal Of High Dilution Resarch, 13(47), 139.
Frei, H. (2014). H1N1 Influenza: A Prospective Outcome Study with Homeopathy and Polarity Analysis. American Journal Of Homeopathic Medicine, 107(3), 114-122.
Frenkel, M. (2010). Homeopathy in cancer care. Alternative Therapies In Health & Medicine, 16(3), 12-16.
Hechavarria Torres, M., Benítez Rodríguez, G., & Pérez Reyes, L. (2014). Efectividad del tratamiento homeopático en pacientes con síndrome depresivo. (Spanish). Medisan, 18(2), 302-308.
Hellhammer, J., & Schubert, M. (2013). Effects of a Homeopathic Combination Remedy on the Acute Stress Response, Well-Being, and Sleep: A Double-Blind, Randomized Clinical Trial. Journal Of Alternative & Complementary Medicine, 19(2), 161-169. doi:10.1089/acm.2010.0636
Hostanska K, Rostock M, Baumgartner S, Saller R. Effect of two homeopathic remedies at different degrees of dilutions on the wound closure of 3T3 fibroblasts in in vitro scratch assay. International Journal Of High Dilution Resarch [serial online]. July 2012;11(40):164-165. Available from: Academic Search Complete, Ipswich, MA. Accessed January 9, 2015.
Jha, C. K., & Madison, J. (2013). Strategies for reinventing and reinforcing the disrupted biography of people with HIV in Nepal. Health Sociology Review, 22(2), 221-232. doi:10.5172/hesr.2013.22.2.221
Kawakami, A. P., Osugui, L., César, A. T., Priven, S. W., de Carvalho, V. M., & Bonamin, L. V. (2009). In vitro growth of uropathogenic Escherichia coli isolated from a snow leopard treated with homeopathic and isopathic remedies: a pilot study. International Journal Of High Dilution Resarch, 8(27), 41-44.
Kay, P. H., Rashid, S., & Panchal, N. (2014). Advances in Homeopathy: Targeting of Health Promoting Genes Using Sequence Specific Homeopathic DNA Remedies. Homoeopathic Heritage, 40(7), 22-24.
Lenger, K., Bajpai, R. P., & Spielmann, M. (2014). Identification of unknown homeopathic remedies by delayed luminescence. Cell Biochemistry And Biophysics, 68(2), 321-334. doi:10.1007/s12013-013-9712-7
Majewsky, V., Scherr, C., Arlt, S. P., Klocke, P., & Baumgartner, S. (2012). Reproducibility of effects of the homeopathic dilutions 14x - 30x of gibberellic acid on growth of Lemna gibba L. International Journal Of High Dilution Resarch, 11(40), 196-197.
Majewsky, V., Scherr, C., Arlt, S. P., Kiener, J., Frrokaj, K., Schindler, T., & ... Baumgartner, S. (2014). Reproducibility of effects of homeopathically potentised gibberellic acid on the growth of Lemna gibba L. in a randomised and blinded bioassay. Homeopathy, 103(2), 113-126. doi:10.1016/j.homp.2013.12.004
Malhi, L., & Saini, R. S. (2012). Homeopathy as an Adjunct to Allopathic Therapy. UBC Medical Journal, 3(2), 32-34.
Marino, F. V. (2012). Homeopathy and Celiac Disease: A Contribution toward Healing. American Journal Of Homeopathic Medicine, 105(1), 4-15.
Medhurst, R. (2013). Homoeopathy for Eczema. Journal Of The Australian Traditional-Medicine Society, 19(2), 104-106.
Mollinger, H., Schneider, R., & Walach, H. (2009). Homeopathic pathogenetic trials produce specific symptoms different from placebo. Forschende Komplementarmedizin, 16(2), 105.
Molski, M. (2010). Quasi-quantum phenomena: the key to understanding homeopathy. Homeopathy, 99(2), 104-112. doi:10.1016/j.homp.2009.11.009
Novosadyuk, T. (2013). Effect of dinamization as a characteristic of potentiation of homeopathic remedies. International Journal Of High Dilution Resarch, 12(44), 86-87.
Peckham, E. J., Nelson, E. A., Greenhalgh, J., Cooper, K., Roberts, E. R., & Agrawal, A. (2013). Homeopathy for treatment of irritable bowel syndrome. The Cochrane Database Of Systematic Reviews, 11CD009710. doi:10.1002/14651858.CD009710.pub2
Piraneo, S., Maier, J., Nervetti, G., Duca, P., Valli, C., Milanesi, A., & ... Nascimbene, C. (2012). A randomized controlled clinical trial comparing the outcomes of homeopathic-phytotherapeutic and conventionai therapy of whiplash in an emergency department. Homoeopathic Links, 25(1), 50.
Posadzki, P., Alotaibi, A., & Ernst, E. (2012). Adverse effects of homeopathy: a systematic review of published case reports and case series. International Journal Of Clinical Practice, 66(12), 1178-1188. doi:10.1111/ijcp.12026
Quak, T., Rudofsky, L., & Dugue, R. (2011). Asthma bronchiale - Verschreibung von Ambra grisea aufgrund eines auffallenden Lokalsymptoms. Allgem Homoopath Zeit, 256(5), 8
Rattan, S. S., & Deva, T. (2010). Testing the hormetic nature of homeopathic interventions through stress response pathways. Human & Experimental Toxicology, 29(7), 551-554. doi:10.1177/0960327110369858
Saeed-ul-Hassan, S., Tariq, I., Khalid, A., & Karim, S. (2013). Comparative Clinical Study on the Effectiveness of Homeopathic Combination Remedy with Standard Maintenance Therapy for Dengue Fever. Tropical Journal Of Pharmaceutical Research, 12(5), 767-770. doi:10.4314/tjpr.v12i5.16
Saha, S. K., Roy, S., & Khuda-Bukhsh, A. R. (2013). Evidence in support of gene regulatory hypothesis: Gene expression profiling manifests homeopathy effect as more than placebo. International Journal Of High Dilution Resarch, 12(45), 162-167.
Sampath, S., Narasimhan, A., Chinta, R., Nair, K. J., Khurana, A., Nayak, D., & ... Karundevi, B. (2013). Effect of homeopathic preparations of Syzygium jambolanum and Cephalandra indica on gastrocnemius muscle of high fat and high fructose-induced type-2 diabetic rats. Homeopathy: The Journal Of The Faculty Of Homeopathy, 102(3), 160-171. doi:10.1016/j.homp.2013.05.002
Siebenwirth, J., Ludtke, R., Remy, W., Rakoski, J., Borelli, S., & Ring, J. (2009). Effectiveness of a classical homeopathic treatment in atopic eczema. A randomised placebo-controlled double-blind clinical trial. Forschende Komplementarmedizin, 16(5), 315.
Stevenson, H. (2010). Breast cancer study: The cytotoxic effects of homeopathic remedies on breast cancer cells. Homeopath Pract, 46.
Teixeira, M. Z. (2011). Scientific evidence of the homeopathic epistemological model. International Journal Of High Dilution Resarch, 10(34), 46-64.
Teixeira, M. Z. (2014). 'Paradoxical pharmacology': therapeutic strategy used by the 'homeopathic pharmacology' for more than two centuries. International Journal Of High Dilution Research, 13(49), 207-226.
Teut, M. (2010). Homeopathic treatment of patients with dementia. Am J Homeopath Med, 103(3), 120.
Thompson, E., Shaw, A., Nichol, J., Hollinghurst, S., Henderson, A., Thompson, T., & Sharp, D. (2011). The feasibility of a pragmatic randomised controlled trial to compare usual care with usual care plus individualised homeopathy, in children requiring secondary care for asthma. Homeopathy, 100(3), 122-130. doi:10.1016/j.homp.2011.05.001
Treuherz, F. (2013). School suffers salmonella outbreak - how one homeopath helped 100 students. Homoeopath, 32(3), 8.
von Hagens, C., Schiller, P., Godbillon, B., Osburg, J., Klose, C., Limprecht, R., & Strowitzki, T. (2012). Treating menopausal symptoms with a complex remedy or placebo: a randomized controlled trial. Climacteric, 15(4), 358-367. doi:10.3109/13697137.2011.597895
Zaidan, S. (2012). Belladonna, Hyoscyamus and Stramonium pharmaceutical drugs or homeopathic remedies. The effect of these plants in treating mental illnesses: A comparative study. Homeopath Int, 2012(2), 12.
Zuzak, T. J., Rauber-Lüthy, C., & Simões-Wüst, A. P. (2010). Accidental intakes of remedies from complementary and alternative medicine in children—analysis of data from the Swiss Toxicological Information Centre. European Journal Of Pediatrics, 169(6), 681-688. doi:10.1007/s00431-009-1087-9
While reading these research publications, you might remind yourself of the reason that I continue to follow my attempt to offer homeopathy despite the odds. That NOT doing so feels like an abandonment of the primary code of conduct as a health practitioner ‘do no harm’ and against following the code ethics within the principles of beneficence and non-maleolence.4 If I don’t offer something that I know can benefit someone’s condition of health; then I feel that I am not acting as the compassionate human being that I know I am. If you would like to find out more, please contact me. I will be happy to conduct further inquiries. My fees are generally at $150.00 per hour for these services but are also listed on my website at www.accessnaturalhealing.com.
REFERENCES:
About 70-80% of patients taking homeopathic treatment for chronic disease report improvement, and in at least one study they prefer it over conventional treatment, according to a collection of studies written up by our friends down under, Homeopathy Plus. Possibly you are aware of the six-year Bristol Homeopathic Hospital study, which showed that out of 6,544 patients with chronic disease, sometimes of many years' duration, 70.7 per cent reported positive health changes.
But there's more.
A study on several alternative health modalities in Northern Ireland shows homeopathy narrowly edging out acupuncture with 79 per cent of patients reporting positive outcomes.
A study carried out at a health clinic in Dorset, England shows 84 per cent of patients reported improvement, and 81 per cent attribute their improvement to homeopathy.
A German study found that most parents with cancer-stricken kids who had them treated homeopathically rated their satisfaction rate as "very high" and would recommend homeopathy to other parents.
A large-scale Swiss study comparing patient satisfaction with homeopathic treatment to conventional medicine for chronic disease showed homeopathy scoring significantly better, with greater improvement and fewer side effects.
Finally, a 103-centre study in Switzerland and Germany followed 3,079 patients over eight years, and found:
* On average, disease severity decreased dramatically and improvements were sustained * Three in ten patients stopped treatment because of major improvement * Mental and physical quality of life scores increased substantially * Biggest and fastest improvements happened for children and the patients who started out the most sick.
Conditions treated ran the gamut, covering both physical and emotional afflictions.
Those who wonder why homeopathy continues to grow in popularity worldwide despite a mechanism of action that defies common "wisdom" and a well-funded and highly-motivated opposition should take note of these studies.
Read the original article, which has more details and full citations, here.
(In another departure, we are reposting this blog by Julie Bailey Obradovic, that originally ran on her personal blog on January 29, 2015. We thought it was an important and eloquent expression of something that many, many parents have in common. )
On November 15, 2002, we went out to celebrate my husband’s birthday. My aunt had kindly offered to watch our two children for us while we celebrated. It was generous of her to do so, and we gratefully took her up on it. We had a wonderful evening . . . until we returned.
She was standing in the hallway just coming down from the stairs of our split-level home as we entered around 1 a.m. Even though it was dark, her face was clear as day, and it was not displaying a good expression. If anything, she looked as if she had just witnessed a horrible tragedy.
Immediately, without asking us about our evening, she urged us to go upstairs and check on our daughter. According to her, our baby had let out a scream unlike she had ever heard only moments before. She truly thought someone had entered the house and had stabbed her, and she was just about to call 9-1-1.
After racing upstairs, she scooped her up out of the crib still mid-scream. The way she described it, Eve was screaming so hard that she couldn’t breathe, her face red with excruciating pain, arching her back as if to fall back into the crib the whole time. Eventually, she stopped, but not in a normal way. She collapsed in my aunt’s arms, as if to pass out. Although still breathing, she wouldn’t wake. My aunt feared she was dying.
Right then, we got home.
Because I didn’t hear the scream, something I have only heard in my dreams since, I couldn’t gauge the seriousness of what had happened accurately. I knew my aunt was the last person to overreact, and given her panic, I realized something was very wrong. We ran upstairs to find Eve just as she had left her, appearing to be sleeping peacefully in her crib.
I called her pediatrician immediately. Eve had been suffering from repeated and chronic ear infections for over 14 months at that time, at least 11 at our last count, and had been on at least that many rounds of antibiotics, each one a stronger, harsher version than the next, none of which ever did anything to alleviate them. In fact, her gums, her lips, her vagina, and her butt were covered in yeast as a result, and patches of eczema were popping up on her elbow and knee creases as well (something that finally cleared with an antifungal).
I suspected she had another ear infection, which often made her scream at night, and tried not to worry too much. I also tried to calm my aunt who said she knew what a baby crying from ear pain sounded like, and this was not it. She was adamant we go to the hospital.
When the doctor finally called back, he believed it was likely ear pain too given her history, told us to give her some pain reliever, and to bring her to the office in the morning. If anything else happened, we were to go to the emergency room, but he didn’t believe it was worthy of a trip right then.
Because over a year’s worth of my instinct that something was seriously wrong with Eve had been disregarded by my pediatricians, and twice, had been criticized for it, I chose to obey the doctor’s orders. I was tired of being made to feel like I was a bad mom by wanting to do other than what they said.
My aunt was upset. She offered to stay overnight with our son if we would just go. She offered to go with me if Matt wanted to stay home. She pleaded. She begged. And when I finally promised to take Eve in the morning first thing, she reluctantly got her coat and said in a way she had never spoken to me, “I have been a mother for 30 years. I was an aunt to you and all of your cousins. I have been around children and babies my whole life. I am telling you, Julie Ann, I have never heard a baby scream like that. Ever. Something is wrong.”
The next day she was not diagnosed with another ear infection. She didn’t have one, but in an effort to try to prevent them, they scheduled her for ear tube surgery. She would have it December 16th, which she did. It did not stop the ear infections that continued for the next two years, and no explanation for the high-pitched, back-arching screaming fit was ever given. It was as if it never happened.
On December 21st, I gave Eve a bath, careful not to get any water in her ears. I was so hopeful that the surgery would put behind the nightmare of illnesses and strange symptoms that had started with an undiagnosed, hot burning rash on her face at one month old, continued with a large, hot, lump on her leg where she received several shots at 4 months old and never went away for weeks, and then finally manifested as one long ear infection beginning at 5 months until now.
Between the constipation interspersed with yellow diarrhea, the eczema, her hair starting to fall out, the gait she was walking with, the incessant drooling around 12 months, and the hypotonia that had developed around 10 months, I had had enough.
Finally, finally, finally, I thought, this would be behind us. Finally, my baby girl would be healthy. No more antibiotics and their side effects. No more nebulizers for respiratory infections. No more covering her ears at the sound of the vacuum or singing. No more prescription creams for skin rashes. No more sleepless nights. No more.
I wrapped Eve in a towel and called Matt to grab the camera. In my newfound sense of relief and hope, I wanted to capture the beginning of a new chapter for her. He met me in her bedroom and together we tried our hardest to make her laugh and smile to get a great photo. (These were the days before digital cameras, and film was not something you wasted.)
Within a few minutes, I realized something I hadn’t until then. Eve had stopped smiling. No matter what we did, no matter how hard we tried, there was nothing, just a vacant, expressionless, unengaged face of angel looking in our direction but not really at us.
Worse, I simultaneously realized, she hadn’t spoken in weeks either. She didn’t have a lot of words that year, but she had words. She pointed, she repeated, and she tried. On the floor of her bedroom that night, actually ever since Matt’s birthday I could prove with video, they were gone.
I quietly asked Matt to put the camera away and got her ready for bed. Without saying a word, I went to my room, turned off the light and lay in the dark on my bed towards the direction of her nursery. Still in my clothes, I stared wide-eyed into the dark, filled with an anxiety that has not left me since.
I knew in that moment . . . I knew in a way that only a mother can know . . . my life, her life, and our baby girl was forever changed, even though I would spend the next two years believing that because a doctor didn’t confirm it, I must be wrong.
A few weeks before Matt’s birthday, Eve received her fourth DT DTP vaccine, her fourth Prevnar vaccine, her third polio vaccine, and her first MMR at the same time. This occurred within days of ending another round of antibiotics. Although we can never prove it because we didn’t go to the hospital that night, nor were the proper tests done the following day, the description of what Eve experienced that night is identical with a condition called “encephalopathy”. That’s a fancy word for brain inflammation and swelling. A high-pitched scream, an arched back, and neurological damage afterwards are a textbook description of the condition.
Here are the symptoms and causes per Medical News Today:
Encephalitis can develop as a result of a direct infection to the brain by a virus, bacterium or fungus (infectious encephalitis, or primary encephalitis), or when the immune system responds to a previous infection; the immune system mistakenly attacks brain tissue (secondary encephalitis, or post-infectious encephalitis).
Primary (infectious) encephalitis: according to the NHS (UK), there are three main categories of viruses: 1. Common viruses, such as HSV (herpes simplex virus) or EBV (Epstein Barr virus). 2. Childhood viruses, such as measles and mumps. 3. Arboviruses, which are spread by mosquitoes, ticks and other insects, and include Japanese encephalitis, West Nile encephalitis and tick-borne encephalitis.
Secondary (post-infectious) encephalitis: could be caused by a complication of a viral infection. Symptoms start to appear days and even weeks after the initial infection. The patient’s immune system treats healthy brain cells as foreign organisms that need to be destroyed, and attacks them. We don’t know why the immune system goes wrong and does this.
Encephalitis is more likely to affect children, elderly people, individuals with weakened immune systems, and people who live in areas where mosquitoes and ticks that spread specific viruses are common.
The package insert of the MMR vaccine lists encephalopathy as a potential, albeit rare, vaccine reaction. So does the DTP. The United States Federal Claims Court for vaccine injuries has also awarded numerous families compensation for children who have suffered encephalopathy following the DTP and MMR, including dozens of children since who have actually been compensated for death caused by the MMR. Yes, per our federal government, more children have been killed by the MMR in the last 10 years than have died from the measles. The threshold of risk-reward benefit appears to have been reached.
Within a year of this episode, I began to research what could possibly be wrong with my daughter and why. Until then, I had implicitly trusted the medical establishment with both of my children’s lives, and my third that was on the way. Even when I doubted their choices, I always did what they told. Always. And when they told me that my daughter was likely not talking because of her brother, and that not all kids crawl, and that it’s normal for kids to shake their heads back and forth, and it’s normal to have constipation for a year, and on and on and on . . . I believed them.
It wasn’t until I had heard about the Homeland Security Act of 2002 and the secret “Lilly Rider” that had been anonymously sneaked in at the 11th hour to protect Eli Lilly and their vaccine preservative Thimerosal from liability (later credited to Dick Armey – R), that I ever, ever, ever questioned vaccines or anything about them. As many people currently believe, I also believed vaccination was a miraculous duty in the modern world. If I needed to get my child a shot at two months old, I was there on that day, no questions asked.
There was no Jenny McCarthy in 2004 when that happened for me. I had no clue who Dr. Wakefield was, what he had published, or how or if that was remotely relevant if at all to my life. There was no Generation Rescue, no Autism Speaks, no Facebook, no Twitter, and very little social media available. At best, you found Yahoo groups where you could gather ideas for research and keep up with the politics. I, like thousands and thousands of other parents across the globe, had to do the research my self.
When my third child was born that year, there were far more questions than answers regarding to what had happened to Eve and why. But within a few months, I learned some frightening things . . . that my brother had had a horrible reaction to the MMR . . . and that my mother, in spite of repeatedly being given it, had never developed immunity . . . and that the measles virus could take up to 30 days to enter the brain upon exposure.
I learned that the symptoms of everything wrong with my daughter were the symptoms of mercury poisoning . . . that mercury had the power to open the blood-brain barrier and allow viruses, bacteria, and other toxins in that should never be there . . . that she had been injected with mercury on the first day of her life . . . that the CDC had studied children who received no mercury in the first month of life and compared them to children who had received 25 mcg or more and discovered there was a 7.7 relative risk of developing autism (and an 8.35 RR of ADHD), and then redid the study four more times over the next four years to get that risk down to 1.52 . . . and then destroyed, lost, or sent the original data sets offshore so they could never be independently analyzed . . . But only after meeting at Simpsonwood, Georgia to figure out how to protect themselves from lawsuits. I learned how they hired the IOM to exonerate them, and how they lied under oath to Congress on July 18, 2000, pretending to know nothing about that which had just been revealed at Simpsonwood . . . which happens to be my anniversary, and the day I confirmed I was pregnant with Eve.
You can read the whole story and download all of the emails and studies and verify everything for yourself here at www.putchildrenfirst.org or by simply reading David Kirby’s award-winning book about the whole debacle, Evidence of Harm, or Dan Olmsted and Mark Blaxill’s meticulous account of the history of mercury in medicine in their book, Age of Autism. Or you can even save yourself all of that time and watch the new documentary “Trace Amounts” www.traceamounts.com somewhere near you in the next few months.
Many journalists and bloggers and doctors have decided the behavior of the CDC is and has been perfectly normal, that it’s perfectly fine for them to investigate themselves and find themselves not guilty, and that the fact that the explosion of neurological disorders in the generation since (all which are symptoms of mercury poisoning . . . ADHD, autism, speech delay, tics) is nothing more than an unfortunate coincidence. That is actually what a doctor said it was to David Kirby on Meet the Press in 2005 . . . “An unfortunate coincidence.”
And so I had a choice that year as my newborn baby came into the world in 2004. Do the same thing I had with Eve and expect a different result? Or take a step back, really investigate what was happening, read all of the science for myself, and wait. Hold off until I knew more?
Crazily, for 6 months, I did the same I had with Eve. I was too afraid to challenge my doctors. Too afraid to leave my baby unprotected. Too afraid to even bring up the corruption being unearthed at the CDC. I vaccinated my baby on time, every time.
And then she got an ear infection, at the exact month as Eve had first gotten hers. I fell to my knees and begged God . . . begged Him . . . that if he would just spare me this daughter . . . that I would do anything in my power to help kids like Eve and to get to the bottom of what had happened. We stopped vaccinating right then and there.
In my worst moments, I wish every condescending, know-it-all parent, journalist, blogger, and citizen who never had to live through what we did . . . never had to make the decisions I had to make . . . never had to learn of the betrayal of their government and medical community on the back of their child like we did . . . never read a study, or the minutes of Simpsonwood . . . never heard of Brick Township, Frederick Wellman, William Miller, Dr. Elizabeth Peabody Trevett, Poul Thorsen, or Willian Thompson and have no idea why they matter . . . the pain of a medically brain injured child.
I wish all of those people the bullying, the vitriol, the isolation, and the hatred of being a parent in my position.
I wish them the suffering of the loss of a child that is still alive. March 27, 2001, I brought a healthy, beautiful, vibrant baby into this world. Over the next 18 months she got sicker and sicker, all the while no one doing anything to make her better, and on November 15, 2002, the daughter I once had . . . the child she was meant to be, basically died. The baby girl I had given birth to was gone, but not.
I wish them a lifetime of regret. A lifetime of never having closure. A lifetime of anxiety and panic and worry. A lifetime of loss and an indescribable, never-ending soul-wrenching heartache that taints every moment of every day for you, no matter how hard you try it not to.
I wish them the pain of going it alone. Of knowing that because your doctors didn’t do the right tests and file the right reports, you will never see a dime.
I wish them a lifetime of watching drug commercials with side effects taking up half the time and then being told the side effects of vaccines don’t exist . . . and that even if they do . . . even IF they do, they condescendingly say . . . it doesn’t matter. Your child was an acceptable loss to society. Some kids gotta die so more may live. Guess you guys pulled the bad straw.
I wish them seeing commercials of lawyers offering to compensate you on that same drug five years later because you can actually sue drug makers for their shoddy work with those drugs. I wish them knowing what it feels like to know they have no such recourse for their child.
I wish them being told they are liars, and dangerous, and public menaces, even though there is not a shred of evidence of that being true in any capacity of their lives.
I wish them the pain of someone they love and trust and care about, someone they think has their back and believes in them, post a factually incorrect, not-even-kind-of-based-in-truth article or graphic on a controversy they have spent 5 minutes reading about but you have spent every day of every year for 10 years immersed in, and realizing all this time you were wrong. They think you’re a misguided lunatic, and it was easier for them to tell you this in a passive-aggressive way on Facebook than to your face.
I wish them sleepless nights and night terrors where you wake drenched in sweat, certain you are being buried alive or doing everything you can to save your child from a fire but can’t kick the door down.
I wish them at least one suicidal thought because the guilt of what happened on your watch and the anger of why and how and the level of betrayal you feel is so deep you see no other way out of the pain for the rest of your life.
I wish them a lifetime of wondering what their child would have been like. Of never being able to attend a school function, a parent teacher conference, or sporting event and not wondering, what if? Of having children the same age in their families and neighborhoods that went unscathed and wondering, why her? Why you? Why not them? Of every milestone of your healthy children being a reminder of your unhealthy child’s plight. Of never having a single moment of joy for one child without instantaneously feeling sadness at the loss of it for the other.
I wish them hoping, begging, pleading that there really is a heaven so that when they die, they finally get to meet that child.
I wish them being told they are a horrible person for even thinking that.
I wish them this and so much more. In my worst moments, there is so much more.
And then I think, no. I don’t wish that. I actually don’t wish this on anyone. I live in the Twillight Zone, one where my reality is not real according to the authorities. Where my pain, my child, her life, and our loss not only didn’t happen, but that it doesn’t matter if it did. No one, not even the people who hate me for simply not wanting to lose another child in the same way and to protect other parents from the same fate, deserve this.
And so then I wish for two more things. Forgiveness and faith. I pray for forgiveness for my evil thoughts. I pray for forgiveness of myself and the people, policies, and programs put in place that led to this disaster.
I pray for the faith that somehow, some way, this will all get worked out and we can do what every single person on either side of the controversy ultimately wants: to protect kids. To RESPONSIBLY and CAUTIOUSLY prevent infectious AND chronic disease.
I pray for the faith that someday my child’s sacrifice in the war on infectious disease will be honored. Just as we honor those that fall at the disease, I pray someday we will acknowledge, honor, and care for those who fell at the hands of friendly fire. They are just as precious.
I pray for the faith that those responsible for this disaster will someday see justice for what they have done, and even more so, for masterfully taking the blame off themselves and pointing it at the families of the victims. Evil genius, I say.
I pray for faith that there is a reason, even if I never get to know what it is, that this had to happen . . . to Eve and to us.
Meanwhile, I kindly ask that if you believe that Matt and I are a menace to society, bad parents, liars, misguided, delusional, desperate, or any such negative connotation, to have the decency to simply unfriend us, and not just on Facebook, but in all areas of our lives.
If you believe we would truly try to hurt a child, allow the world to explode in infectious disease, or follow quackery, unfriend us.
If you have failed to do your research and do not know that there is a whistleblower lawsuit against Merck right now, by two of their own virologists who claim they were asked to lie about the true efficacy of the MMR vaccine (basically, it’s not working well anymore), unfriend us.
If you believe that we owe you or society the potential loss of the quality of our youngest daughter’s life by exposing her to the same medical procedures that resulted in the actual loss of the quality of our eldest’s, unfriend us.
If you think that didn’t happen to Eve, unfriend us.
If you think you know more about what happened to our daughter than we do because you watched an Upworthy or Penn and Teller video, unfriend us. (Funny, we’re not supposed to listen to celebrities in this issue unless they hold a certain position I guess.)
If you think continuing to inject a pregnant woman, infant, child, or anyone for that matter with a neurotoxin made by Eli Lilly, that has never . . . not even to this day . . . been tested for safety, not to mention was deemed too toxic for dog vaccines way back in 1935 . . . is an inconsequential responsible health policy, unfriend us.
“We have obtained marked local reaction in about 50% of the dogs injected with serum containing dilutions of Merthiolate (Thimerosal). Merthioiate is unsatisfactory as a preservative for serum intended for use on dogs.”(Director of Biological Services, Pittman-Moore Company, letter to Dr. Jamieson of Eli Lilly Company dated 1935. U.S. Congressional Record, May 21, 2003, E1018, page 9).
If you think the Bush Administration and the CDC could/can be trusted where autism is concerned and have behaved ethically and reliably, and that parents of sick kids, the ones who did exactly as they were told and have no other agenda than to help you protect your own children are the real enemies, unfriend us.
If you think you have the right to judge my family members, siblings, best friends, neighbors, colleagues, and acquaintances who were eyewitnesses to the loss of our child, to our heartache, and will testify to our character and have chosen to take a different path to protect their own children as a result, unfriend us.
And finally, if you think that it’s okay for some children to die so that more may live, I kindly ask that instead of shaming parents who have already given society a child and have decided, “You know what? I’m not giving you another one, and I’m not even going to take a chance on that,” that you reach out them.
I believe the words you are actually looking for for these parents, instead of “stupid,” “misguided,” “maniacs,” “public menaces,” “criminal” and more hateful choices, are “thank you.”
Thank you, for giving your child to the war on infectious disease. Thank you, for taking one for the team. Thank you, for dealing with an insensitive society who has never acknowledged your sacrifice, let alone offered to help you care for your child.
Thank you.
And most important, thank you to the child who gave her life to the effort. Thank her.
Those are the words you should be using. But be prepared. They probably won’t be returned with, “You’re welcome.”
I know I wouldn’t say it. Neither would my daughter. I’m positive she would have preferred her life to have been preserved, as she often now asks me, “Why I am different? Why is it so hard for me to fit in?”
No, I would have never, ever, ever given you or any other person on the planet my child had I been asked. Never. I vaccinated my child to protect her, not you or anybody else.
And deep down inside, as condescending and self-righteous and self-assured as you may be about what you think you know and why you know it and why I’m wrong, you know you are the same.
You know that you would never offer up your child to the greater good either if they asked for her, and you know you wouldn’t dare take that chance with another one of your children if you were in my shoes.
You just have the luxury of never having had to make that choice or live this life.
You should say, “Thank you” for that too.
~ Julie Bailey Obradovic
http://thinkingmomsrevolution.com/believe-words-youre-looking-thank/
scientific community covid 19 italian homeopathy


